Fig. 54.1
Mid-esophageal short axis view of aortic valve showing vegetation on aortic leaflets. Arrows showing vegetation on aortic valve leaflets
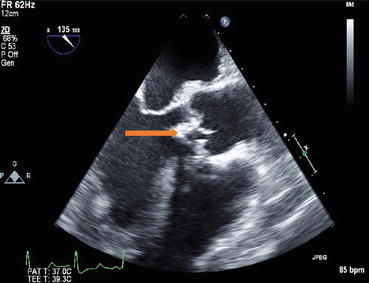
Fig. 54.2
Mid-esophageal long axis view of aortic valve showing mobile vegetation on aortic valve. Arrow showing vegetation on aortic valve leaflet. Valve viewed in long axis
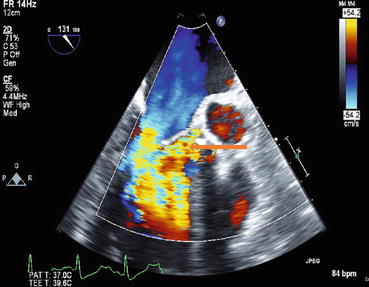
Fig. 54.3
Mid-esophageal long axis view with color Doppler in a patient with aortic valve endocarditis showing severe regurgitation at the aortic valve
Questions
- 1.
What are the risk factors for infective endocarditis?
- 2.
Explain the pathophysiology of infective endocarditis?
- 3.
Describe the clinical manifestations of infective endocarditis?
- 4.
How do you diagnose infective endocarditis?
- 5.
What is the role of TTE and TEE in the diagnosis of infective endocarditis?
- 6.
What are the treatment options for patients with infective endocarditis?
- 7.
Which are the guidelines on managing high-risk patients presenting for surgery?
Answers
- 1.
The following patients present a high risk for infective endocarditis [1–9]:
- (a)
Male, elderly (age > 60)
- (b)
Prior history of prior IE
- (c)
Poor dental hygiene
- (d)
Patient undergoing dental procedures involving gingival tissues
- (e)
Patients with valvular heart disease (e.g., rheumatic valvular disease)
- (f)
Patients with uncorrected or partially corrected congenital heart disease
- (g)
IV drug use
- (h)
Prosthetic valves
- (i)
Immunosuppressed patient
- (j)
Patients with history of diabetes
- (k)
Patients with intracardiac devices
- (l)
Patients undergoing hemodialysis
- (a)
- 2.
Pathophysiology:
- (a)
IE occurs when bacteria or fungi invade sterile platelet-rich thrombus at sites of injury in the endocardium.
- (b)
Sources of bacteria include the skin, oral cavity, mucosal surfaces, or sites of focal infection.
- (c)
Infection results in invasion of the thrombus and destruction of the underlying valvular and endocardial tissues.
- (d)
Bacteria usually resistant to the complement system of the body.
- (e)
Common bacterial species: Staphylococcus, Streptococcus, Enterococci, and HACEK group (Haemophilus, Actinobacillous, Corynebacterium, Eikenella, and Kingella).
- (a)
- 3.
Infective endocarditis can affect all organ systems of the body [1–9]:
- (a)
Nonspecific symptoms: fever (most common symptoms), chills, sweats, headaches, weight loss, back pain, myalgia arthralgia, cough, and pleuritic chest pain
- (b)
Other symptoms highly specific for IE: cardiac murmur (85% of patients), splinter hemorrhage in nail beds, petechiae on skin and mucous membranes, Janeway lesions (nontender macules on palm and sole), Roth spots (hemorrhagic lesions on retina), and Osler nodes (tender nodules on fingers and toes)
- (c)
Cardiac complications: valvular insufficiency, congestive heart failure (30–40% of IE patients), and periannular and intraventricular abscesses (can result in intracardiac fistulas), cardiac arrhythmias (usually the result of periannular abscesses)
- (d)
Vascular-embolic complications: septic emboli (15–35% of IE patients), mycotic aneurysm, and vertebral osteomyelitis
- (e)
Neurologic complications (mostly from vascular embolic events): brain abscess, embolic stroke, and cerebral hemorrhage
- (f)
Renal complications: kidney infarct from septic emboli and glomerulonephritis (caused by immune complexes)
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


- (a)


