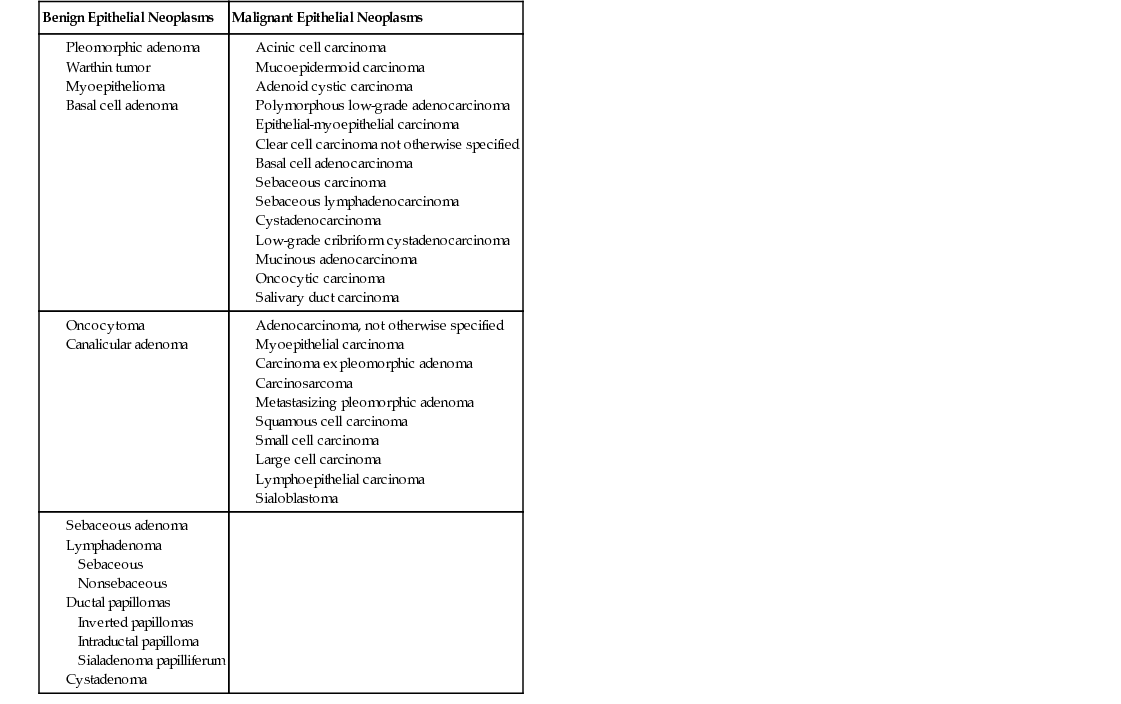
Lisa M. O’Neal The salivary glands include the paired parotid glands, the submandibular and sublingual glands, and numerous minor salivary glands found in the upper aerodigestive tract; these glands produce saliva to aid in the breakdown of food. Diseases that affect the salivary glands are divided into neoplastic and non-neoplastic categories. The non-neoplastic category is further divided into infectious and noninfectious origins; neoplastic diseases are either benign or malignant. Acute suppurative sialadenitis (bacterial parotitis) is covered in Chapter 99.1 Salivary gland infections are found in all age groups and populations. However, malfunction of the salivary gland is most common in adults and typically involves a decrease in the production of saliva.1 Malignant neoplasms involving the salivary glands account for less than 5% of all head and neck tumors, not including skin cancers.2 The distribution of salivary tumors is more common among men than women.3 Salivary tumors can occur at any age, and the risk of developing a salivary gland cancer increases with age. The average age at time of diagnosis is 64 years.3 Salivary tumors in older adults most commonly affect the parotid glands. Radiation treatment to the head and neck and workplace exposure to certain radioactive substances increase one’s risk of developing a salivary gland cancer.3 Several studies have identified an increased incidence of breast cancer in patients who have had mucoepidermoid carcinoma (MEC) of the salivary glands, and an increase in minor salivary gland adenocarcinoma has been associated with occupational exposure to woodworking and to furniture, boot, and shoe manufacturing.3 There does not appear to be any increased incidence of salivary gland cancer from inheritance or in individuals with a history of family members with salivary gland cancer.3 Recent studies have shown that a diet low in vegetables and high in animal fat may increase one’s risk for developing salivary gland cancer.3 Cell phone usage was shown in a singular study to increase the risk of developing benign parotid gland tumors. However, other studies have shown no relation; research is still ongoing.3 Recurrent parotitis, sialolithiasis (salivary gland stones), branchial cleft anomalies, Sjögren syndrome, xerostomia, ptyalism (hypersalivation), sialosis, and benign lymphoepithelial lesion of Godwin are classified as noninfectious salivary gland disorders. Sialectasis (dilation of a salivary duct, either acquired or congenital) can lead to recurrent parotitis. Dilation of the duct and gland can be produced by either stone formation or strictures. Sialolithiasis, which mainly affects the submandibular glands, refers to the formation of stones or calculi in the glands. The stones are predominantly hydroxyapatite, and there may be more than one.4 The higher mucin content of the saliva produced in the submandibular glands, combined with an antigravity flow of saliva, contributes to stone formation.5 The stagnant saliva in the gland also leads to the formation of stones. Elevated serum levels of calcium and phosphorus are not associated with stone formation.5 First branchial cleft anomalies affect the salivary glands, primarily the paired parotid glands. Infected cysts and sinus tracks associated with these anomalies usually are initially seen in the preauricular area and can affect the facial nerve.4 Sjögren syndrome is an autoimmune disorder that affects the salivary glands. On pathologic evaluation, a lymphocytic infiltrate with acinar atrophy, ductal epithelial hyperplasia, and metaplasia can be found. Benign lymphoepithelial lesion of Godwin is an inflammatory condition often found in association with human immunodeficiency virus (HIV) infection. It can be confused pathologically with malignant lymphoma, metastatic carcinoma, sarcoidosis, or chronic sialadenitis.6 Xerostomia means dry mouth. Several diseases as well as radiotherapy and drug therapy cause these symptoms. The production of excess saliva is called ptyalism; drug treatments (atropine) and other medical conditions are usually the underlying causes.1 Sialosis refers to bilaterally recurring salivary gland edema. Acinar cell hypertrophy, interstitial edema, and striated duct atrophy may be present on pathologic examination. Alcoholism, metabolic disorders such as diabetes and various vitamin deficiencies, obesity, and malnutrition also initiate enlargement of the salivary glands. Certain drugs, including the phenothiazines, heavy metals, thiourea, and iodide-containing substances, cause salivary gland enlargement as a result of their cholinergic effects.1 Infectious diseases that affect the salivary glands include mumps parotitis and other viral infections, syphilis, HIV infection, and granulomatous diseases. Granulomatous diseases affecting the salivary glands include tuberculosis, sarcoidosis, cat-scratch disease, uveoparotid fever (Heerfordt syndrome), and actinomycosis.4 Neoplastic changes also affect the salivary glands. Studies have shown that 2% to 4% of all head and neck neoplasms are salivary gland tumors.4 The majority (70%) of salivary gland tumors involve the paired parotid glands,7 whereas, 8% of salivary gland tumors are found in the submandibular glands and 22% in the minor glands.4 Benign tumors that involve the salivary glands have been classified by the World Health Organization (WHO) into 13 subtypes (Table 96-1). Because of the epithelial and myoepithelial tissue components of the salivary glands, the tumors are defined by their dominant tissue type.4 Of the benign tumors, pleomorphic adenoma (PA) is the most common and is most frequently found in the parotid gland. Warthin tumor, also known as adenolymphoma, is the second most common benign neoplasm of the salivary glands; this tumor is cystic and is found solely in the parotid glands.4 Recent studies have questioned whether or not Warthin tumors are truly parotid neoplasms, but rather a disease of the parotid lymph nodes.4 TABLE 96-1 WHO Classification of Epithelial Salivary Gland Neoplasms The remaining subtypes of benign epithelial tumors make up approximately 15% of all tumors.4 Diagnosis is dependent on definitive histology of the benign neoplasm.4 Malignant tumors of the salivary glands have been classified by WHO into 24 subtypes (see Table 96-1). The parotid gland is the most common site for metastatic disease. The majority (60% to 70%) of patients will have MEC, adenoid cystic carcinoma, acinic cell carcinoma, or polymorphous low-grade adenocarcinoma.4 MECs are the most common cancers of the major and minor salivary glands and are most commonly seen in the parotid gland. Furthermore, MEC has been found to have a strong predilection for the lower lip.8 The majority of MECs are low or intermediate grade and can be surgically treated. However, if the MEC is high grade, there is greater potential for metastasis.4 Adenoid cystic carcinoma accounts for approximately 10% of the malignant salivary gland tumors overall, but 30% of the minor salivary gland tumors.4 These types of tumors often manifest with a nerve palsy because of their predilection for perineural spread. Prognosis after 10 to 15 years is poor (mortality 80% to 90%) because of metastases to other organs.4 Acinic cell carcinomas are found predominately (80%) in the parotid gland and are slow growing. They can occur in both parotids and can metastasize to the cervical lymph nodes.4
Diseases of the Salivary Gland
Definition and Epidemiology
Pathophysiology
Benign Epithelial Neoplasms
Malignant Epithelial Neoplasms
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


