Fig. 47.1
(a) Interventions performed in the Italian RICU according to the two national surveys in 1997 and 2007. Differences for each intervention were statistically significant (p <0,05) between 1997 and 2007 (Modified from [14]). (b) Distribution of interventions in the surveyed RICUs in 2007 according to the level of care (modified from [5]). Differences between the three levels of RICU care were statistically significant for all interventions (p <0.05) except weaning in RIICUs vs RICUs. RMU respiratory monitoring unit, RIICU respiratory intermediate intensive care unit, RICU respiratory intensive care unit
The 2007 AIPO survey has clearly shown that the different attitude of the Italian RICUs in performing weaning activities depends essentially on two factors: (1) the level of respiratory care available (intensive, intermediate, monitoring) and (2) the type of location (acute care hospital , rehabilitative Institute). Concerning the first aspect, weaning-correlated problems have been the cause of admission in 25 % of cases in RICUs providing higher levels of assistance (intensive and intermediate) versus 10 % of the admissions observed in the monitoring units (Fig. 46.1b). As regards the second aspect, the survey has shown that the RICUs located in the acute care hospitals (80 % of the total surveyed units) work largely as step-up units for supporting NIV patients with ARF/ACRF transferred from emergency departments and general wards, whereas they function less frequently as step-down units for difficult-to wean patients coming from ICUs. Conversely, the RICUs set up within rehabilitative centers (20 % of the total surveyed units) work primarily as step-down units of intermediate level in favor of the ICUs belonging to the surrounding acute care hospitals. These RICUs act as weaning and rehabilitative centers for prolonged invasively ventilated patients, most of them having a tracheostomy tube [5, 6]. In accordance with these data is the 1-year experience of one expert RICU showing a rehabilitative vocation that analyzed the interventions performed on 96 patients: 65 % of them came from ICUs and 42 % of them were admitted for prolonged weaning [11]. Likewise, according to a retrospective study [12] including more than 3,000 patients in the period 1990–2005 in five Italian RICUs working as step-down units, the management of prolonged weaning was the cause of the admission in 66 % of cases.
47.4 Models
In Italy, there are two main organizational patterns for the management of patients with prolonged weaning within the pulmonologist’s rehabilitative critical area (Fig. 46.2).
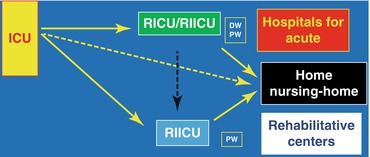
Fig. 47.2
Different clinical models for the care of patients with weaning problems in Italy. ICU intensive care unit, RIICU respiratory intermediate intensive care unit, RICU respiratory intensive care unit, DW difficult weaning, PW prolonged weaning
The first clinical pathway involves the transfer of ventilator-dependents patients into the eight RICUs with “rehabilitative attitude” where long-term (>30 days) multidisciplinary interventions may be applied. The role played by these units is oriented first to recovering as much as possible of the patient’s functional autonomy, from ventilation to neuromotor activities, and, then, to activate home-care programs for patients who remain partly or totally dependent on mechanical ventilation [12–14]. The weakness of this model is due to the small number of these rehabilitative RICUs scattered throughout the national territory and their location in institutions lacking ICU facilities. The latter may have negative implications for safety in case of multiorgan deterioration of the patient during the weaning process.
The second clinical option is based on the transfer of patients with difficult/prolonged weaning into the 36 RICUs located inside acute care hospitals, where the strategy followed to achieve the maximum ventilatory autonomy could be applied for a shorter period of time (<30 days) [5, 14]. In case of failure of further weaning attempts in these acute RICUs, patients could be transferred, if one is available in their regional area, to a rehabilitative RICU. Otherwise, the length of stay in the acute RICU is likely to be extended with the consequence of a reduced turnover of beds available for the admission of new ARF/ACRF patients. The integrated sequential activity of a RICU located in an acute care hospital with that of a weaning center implemented in a close rehabilitative center was the subject of a pilot experience in Tuscany. In a sample of 49 tracheostomized ventilator-dependent patients who were transferred from the ICU to the acute RICU of the same hospital, the passage from the second to the third step of care improved the success rate of weaning from 67.3 to 79.6 % with a positive economic impact [13].
The number of RICUs surveyed nationwide being, unfortunately, still insufficient, a third clinical option involves a prolonged stay of yet unweaned patients in the ICU with negative consequences in terms of efficiency of the resource management system.
47.5 Resources
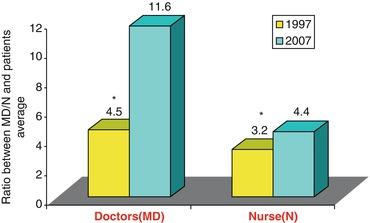
The importance of allocating enough human resources in a weaning center is highlighted by the finding of a very high nursing workload required to manage patients with weaning problems during the first 2 days of admission into an Italian rehabilitative RICU [15]. Unfortunately, the “snapshot” of the Italian RICUs has clearly pointed out that, in the last decade, there has been a contraction in the amount of human resources, in terms of doctor- and nurse-to-patient ratio, albeit without a significant variation in the instrumental resources for monitoring and mechanical ventilation [5, 6] (Fig. 46.3). Moreover, despite the important role of respiratory physiotherapy in critically ill patients, surprisingly, the physiotherapist-to-patient ratio in the RICUs surveyed in 2007 was less than 1:11 for all levels of care units, a value that is lower than the ratio of 1:6 recommended by the AIPO document [2]. Similar results emerged from a retrospective multicenter study conducted in five rehabilitative RICUs [12]. According to this analysis, the reduced doctor-to-patient ratio observed from 1990 to 2005 was associated with a prolonged length of stay, a lower rate of weaning success, and fewer patients dischargeable to home.
 Predictive Models of Prolonged Mechanical Ventilation and Difficult Weaning
Postoperative Continuous Positive Airway Pressure (CPAP)
Noninvasive Mechanical Ventilation in Postoperative Spinal Surgery
BiPAP for Preoxygenation During Reintubation in Acute Postoperative Respiratory Failure
Discharge Planning of Neuromuscular Patients with Noninvasive Mechanical Ventilation After Difficult Weaning from Invasive Mechanical Ventilation: From ICU to Home Care
Noninvasive Ventilation and Weaning Outcome
Predictive Models of Prolonged Mechanical Ventilation and Difficult Weaning
Postoperative Continuous Positive Airway Pressure (CPAP)
Noninvasive Mechanical Ventilation in Postoperative Spinal Surgery
BiPAP for Preoxygenation During Reintubation in Acute Postoperative Respiratory Failure
Discharge Planning of Neuromuscular Patients with Noninvasive Mechanical Ventilation After Difficult Weaning from Invasive Mechanical Ventilation: From ICU to Home Care
Noninvasive Ventilation and Weaning Outcome




Related posts:
Predictive Models of Prolonged Mechanical Ventilation and Difficult Weaning
Postoperative Continuous Positive Airway Pressure (CPAP)
Noninvasive Mechanical Ventilation in Postoperative Spinal Surgery
BiPAP for Preoxygenation During Reintubation in Acute Postoperative Respiratory Failure
Discharge Planning of Neuromuscular Patients with Noninvasive Mechanical Ventilation After Difficult Weaning from Invasive Mechanical Ventilation: From ICU to Home Care
Noninvasive Ventilation and Weaning Outcome
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
