A sensitive way to evaluate for intra-abdominal injury in the trauma patient
![]() In Blunt Trauma
In Blunt Trauma
![]() Unexplained hypotension
Unexplained hypotension
![]() Concern for injury but no obvious indication for laparotomy and serial abdominal examinations are not practical (i.e., unconscious or under anesthesia)
Concern for injury but no obvious indication for laparotomy and serial abdominal examinations are not practical (i.e., unconscious or under anesthesia)
![]() Equivocal focused abdominal sonography for trauma (FAST) examination and concern for an intra-abdominal injury
Equivocal focused abdominal sonography for trauma (FAST) examination and concern for an intra-abdominal injury
![]() Patient unsuitable for computed tomography (CT) in whom there is concern for intra-abdominal injury
Patient unsuitable for computed tomography (CT) in whom there is concern for intra-abdominal injury
![]() Concern for mesenteric or hollow viscous injury not seen on CT
Concern for mesenteric or hollow viscous injury not seen on CT
![]() In Penetrating Trauma
In Penetrating Trauma
![]() Anterior abdominal stab wound and evidence of fascial penetration in the stable patient with no obvious indication for laparotomy
Anterior abdominal stab wound and evidence of fascial penetration in the stable patient with no obvious indication for laparotomy
![]() To evaluate for hollow organ or diaphragmatic injury in the stable patient
To evaluate for hollow organ or diaphragmatic injury in the stable patient
CONTRAINDICATIONS
![]() Absolute Contraindications
Absolute Contraindications
![]() Indication for an emergent laparotomy
Indication for an emergent laparotomy
![]() Relative Contraindications
Relative Contraindications
![]() Prior abdominal surgery
Prior abdominal surgery
![]() Second or third trimester of pregnancy—consider open technique with supraumbilical approach
Second or third trimester of pregnancy—consider open technique with supraumbilical approach
![]() Morbid obesity
Morbid obesity
![]() Significant ascites
Significant ascites
![]() Coagulopathy
Coagulopathy
![]() General Basic Steps
General Basic Steps
![]() Prepare patient
Prepare patient
![]() Analgesia
Analgesia
![]() Technique
Technique
![]() Open
Open
![]() Incision
Incision
![]() Dissection
Dissection
![]() Incise fascia, then peritoneum
Incise fascia, then peritoneum
![]() Place dialysis catheter
Place dialysis catheter
![]() Closed
Closed
![]() Needle into abdomen
Needle into abdomen
![]() Thread guidewire
Thread guidewire
![]() Small skin incision
Small skin incision
![]() Thread dialysis catheter
Thread dialysis catheter
![]() Aspirate
Aspirate
![]() Lavage/Drainage of fluid
Lavage/Drainage of fluid
![]() Analysis of fluid
Analysis of fluid
LANDMARKS
The incision should be made in the midline, one-third of the way between the umbilicus and pubic symphysis. In the pregnant patient or the patient with a pelvic fracture, the incision should be made in the midline, just above the umbilicus (FIGURE 16.1).
SUPPLIES
![]() 1% Lidocaine with epinephrine, 20 mL with 25-gauge needle, 10-mL syringe
1% Lidocaine with epinephrine, 20 mL with 25-gauge needle, 10-mL syringe
![]() Sterile towels or drapes, sterile gown and gloves, mask, and eye protection
Sterile towels or drapes, sterile gown and gloves, mask, and eye protection
![]() Povidone–iodine (Betadine) solution or chlorhexidine
Povidone–iodine (Betadine) solution or chlorhexidine
![]() 11-Blade scalpel
11-Blade scalpel
![]() Syringe and needle (for closed technique)
Syringe and needle (for closed technique)
![]() Flexible guidewire (for closed technique)
Flexible guidewire (for closed technique)
![]() Two clamps and two retractors (for open technique)
Two clamps and two retractors (for open technique)
![]() Peritoneal catheter
Peritoneal catheter
![]() 1 L warm saline for infusion (for lavage)
1 L warm saline for infusion (for lavage)
![]() Tubing to let lavage fluid drain
Tubing to let lavage fluid drain
![]() Suture (for open technique)
Suture (for open technique)
TECHNIQUE
![]() Preparation
Preparation
![]() Place a Foley catheter (unless contraindicated)
Place a Foley catheter (unless contraindicated)
![]() Place a nasogastric tube (unless contraindicated) to suction to decompress the stomach
Place a nasogastric tube (unless contraindicated) to suction to decompress the stomach
![]() Gather all instruments and sterile gown/gloves
Gather all instruments and sterile gown/gloves
![]() Sterilize the abdomen from costal margin to pubis and from flank to flank with povidone–iodine solution (Betadine) or chlorhexidine
Sterilize the abdomen from costal margin to pubis and from flank to flank with povidone–iodine solution (Betadine) or chlorhexidine
![]() Drape the area with sterile towels or drapes
Drape the area with sterile towels or drapes
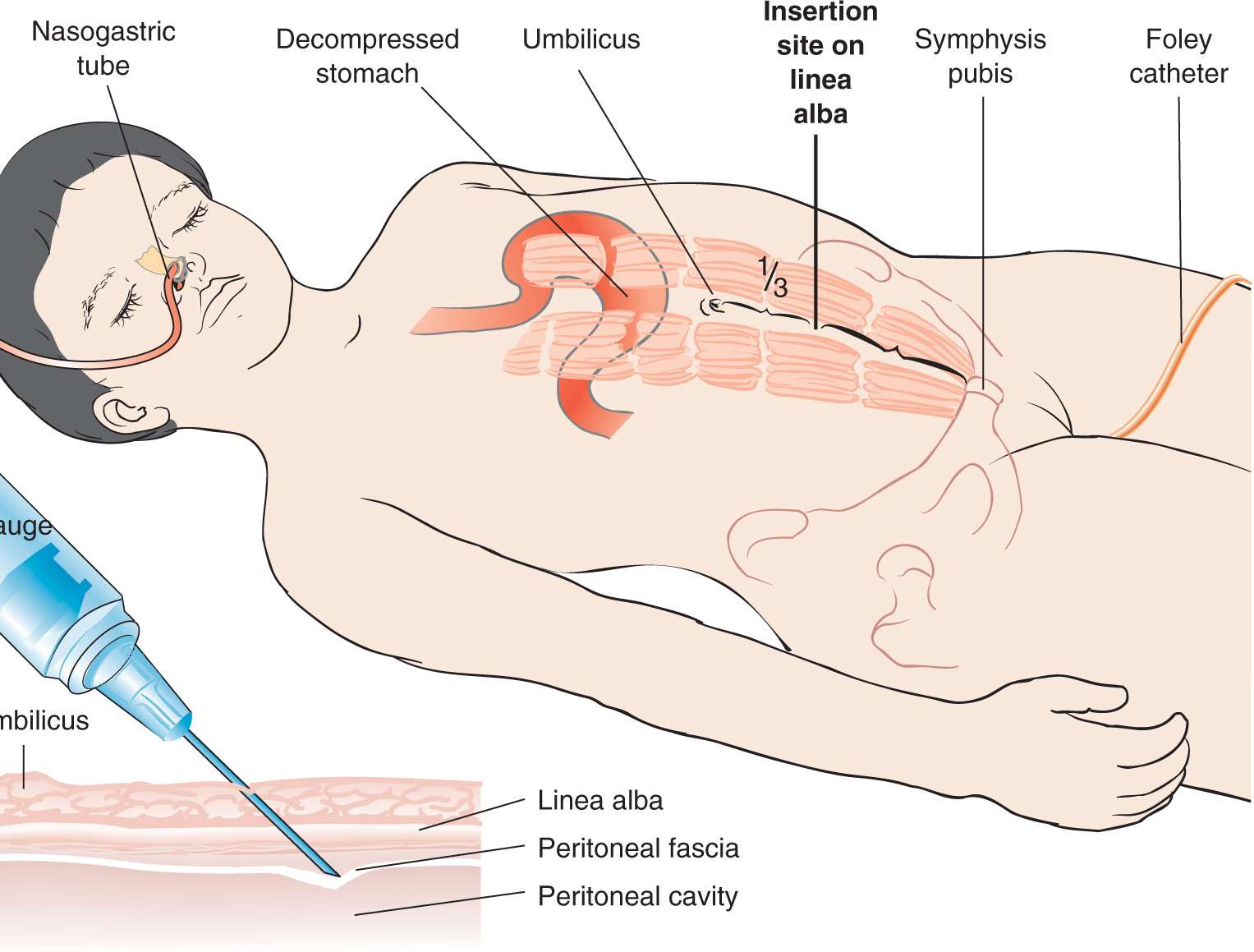
FIGURE 16.1 Anatomical landmarks for diagnostic peritoneal lavage. (From VanDevander PL, Wagner DK. Diagnostic peritoneal lavage. In: Henretig FM, King C, eds. Textbook of Pediatric Emergency Procedures. Philadelphia, PA: Williams & Wilkins; 1997:358, with permission.)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


