Methanol
Uremia
Diabetic Ketoacidosis
Propylene Glycol
Paraldehyde
Propofol
Infection
Iron
Isoniazid
Inborn Errors of Metabolism
Lactic Acidosis
Ethylene Glycol
Salicylates
Starvation ketoacidosis
Question
How would you proceed in the management of this patient?
Answer
The combination of altered mental status, progressive development of a high anion gap acidosis and the presence of a marked osmolal gap are highly suggestive of toxic alcohol ingestion, either methanol or ethylene glycol. Methanol is a common ingredient in windshield washer fluid and ethylene glycol is commonly found in antifreeze. Ingestion of isopropyl alcohol, the third common toxic alcohol ingestion, elevates the osmolar gap but does not result in an acidosis or significant elevation of the anion gap.
Given her decline in mental status and progressive failure of oxygenation secondary to development of pulmonary edema, she was intubated and mechanically ventilated. A loading dose of 15 mg/kg intravenous fomepizole treatment was immediately initiated to prevent further metabolism of the parent alcohol. The cofactors thiamine and pyridoxine were given. Her developing acidosis suggested that she had already metabolized a substantial portion of the parent alcohol into its toxic metabolites, and nephrology was consulted for emergent hemodialysis. Gas chromatography for toxic alcohols returned several hours later and revealed an ethylene glycol level of 257 mg/dL. Repeat urinalysis demonstrated calcium oxalate crystalluria (Fig. 8.1).
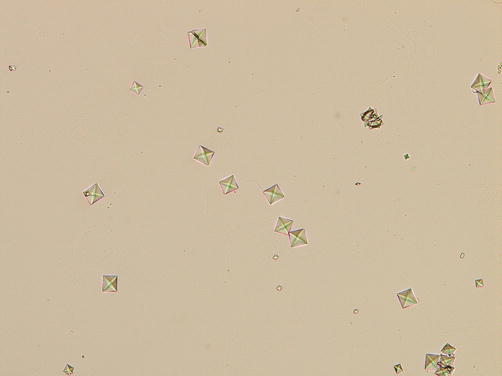
Fig. 8.1
Calcium oxalate crystals
The patient underwent three runs of intermittent hemodialysis and was continued on IV fomepizole per protocol. Her gap acidosis normalized and her measured ethylene glycol fell below 20 mg/dL. Her renal function remained normal throughout her clinical course. Her pulmonary edema resolved and she was extubated on hospital day #2.
Principles of Management
Diagnosis
Ethylene glycol is an organic alcohol with multiple commercial and household purposes, and is typically the primary compound found in antifreeze. It is a colorless liquid, although dyes are often added by the manufacturer. The taste of ethylene glycol is often described as “sweet”, and therefore young children frequently fall victim to inadvertent ingestions [1]. Ethylene glycol is rapidly absorbed by the GI tract and clinical intoxication may be apparent within 20–30 min. Peak serum concentrations can be expected between 1 and 4 h post-ingestion [2]. Ingestions of as little as 1 mL/kg may lead to toxic serum concentrations [3].
Diagnosing ethylene glycol poisoning can be quite challenging, as the acute clinical presentation is typically non-specific and may appear quite similar to ethanol intoxication. Individuals with intentional ingestions may not be forthcoming, or may be too obtunded to provide a history of ingestion. Prompt initiation of treatment is imperative, and delays strongly correlate with the development of acidosis and renal failure once toxic metabolites accumulate (Fig. 8.2) [4, 5]. The gold standard for diagnosis uses gas chromatography to measure serum ethylene glycol levels, but may take 2–4 h to perform, and is not readily available at most medical facilities [2, 6]. Serum measurement of the glycolic acid metabolite has also been advocated by some, owing to its stronger correlation with the development of renal complications, but this also requires gas chromatography and therefore carries the same limitations [7]. Therefore, the clinician often must utilize surrogate markers when considering a toxic alcohol exposure.
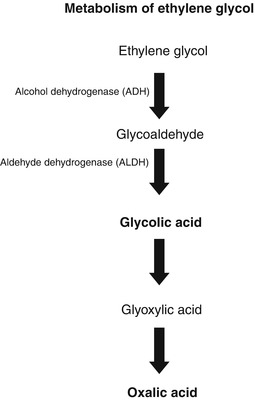
Fig. 8.2
Metabolism of ethylene glycol
Since ethylene glycol is an osmotically active substance, the osmolal gap (measured osmoles – calculated osmoles) will typically be elevated during the initial phase following substantial ingestions. As the parent compound is metabolized, the osmolal gap will gradually decline and a metabolic anion gap acidosis will develop (Fig. 8.3) [9]. There are several caveats to note when interpreting an osmolal gap, however. Numerous formulas exist for calculating serum osmoles, and there is no consensus on which one is superior [2, 10, 11]. One commonly used formula is as follows:
![$$ \mathrm{Osmc}=\left[2\times \mathrm{Na}+1.15\left(\mathrm{glucose}/18\right)+\mathrm{BUN}/2.8 + \mathrm{EtOH}/4.6\right] $$](/wp-content/uploads/2017/07/A329322_1_En_8_Chapter_Equb.gif)
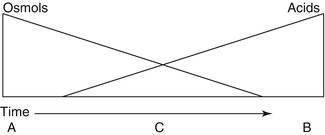
Fig. 8.3
The mountain: A visual schematic for clarifying the temporal relationship between the anion gap and osmole gaps in toxic alcohol poisoning. A: Ethylene glycol is the predominate form in the serum. Only an osmolar gap is present. No acidosis or anion gap yet noted. C: Ethylene glycol is being metabolized. Some glycolic acid is present. Both an osmolar gap and an anion gap acidosis are present. B: All the ethylene glycol has been metabolized to glycolic acid. Osmolar gap no longer exists. Large anion gap acidosis is present (From Mycyk and Aks [8]. Reprinted with permission from Elsevier Limited)
An elevated osmolal gap is non-specific and may be seen with various conditions including ethanol intoxication, alcoholic ketoacidosis, DKA, renal failure, shock, and after use of other exogenous osmotically active compounds such as mannitol [10]. Additionally, since the normal reference range for a calculated osmolal gap may be as low as −10 mosm, the addition of measured osmoles from a toxic alcohol may not raise this gap beyond the accepted upper limit of +10 mosm. This can be understood when considering that an ethylene glycol level of 21 mg/dL (the threshold where treatment is recommended) would only be expected to increase serum osmoles by 4 mosm [2]. Despite these limitations, a large retrospective analysis suggested that an unexplained osmolal gap exceeding 50 was highly suggestive of a toxic alcohol ingestion, and that nearly 50 % of toxic ingestions had osmolal gaps greater than 30 [10].
In the initial phase following ethylene glycol poisoning, the anion gap is typically normal, and then begins to rise approximately 3 h post-ingestion [2]. When presentation or treatment is delayed, the parent alcohol is metabolized by alcohol dehydrogenase and aldehyde dehydrogenase into glycolic acid. Further metabolism of glycolic acid is very slow and therefore this compound progressively accumulates resulting in an anion gap acidosis. Cardiopulmonary manifestations are likely both due to the acidemia, as well as the direct toxic effect of glycolic acid. During this phase, patients may develop tachycardia, hypotension, myocardial depression and congestive heart failure, cerebral edema, and an ARDS-type picture [3, 12].
A small portion of glycolic acid is then further metabolized into oxalate. Deposition of calcium oxalate crystals in renal tubules results in tubular necrosis and renal failure, and generally occurs 24–72 h post-ingestion. This can also lead to significant hypocalcemia [2]. Testing for calcium oxalate crystalluria as an adjunct to the diagnosis of ethylene glycol ingestions has been evaluated. Unfortunately, crystals are seen in only 33–63 % of those with known ingestions, and the baseline prevalence of crystalluria due to other causes such as dietary factors make this finding neither sensitive nor specific [2, 13].
Urine fluorescence is another strategy that has been evaluated by investigators to aid in determination of ethylene glycol ingestions. Fluorescein is often added to engine coolants by manufacturers to facilitate a mechanic’s ability to detect radiator leaks using UV light [2]. In the setting of ingestions, fluorescein is excreted unchanged in the urine. However, not all antifreeze preparations contain this compound. Furthermore, fluorescence is short-lived during the first few hours and may be difficult to detect. Inter-rater reliability when assessing urinary fluorescence is poor and fluorescein cannot be detected when urinary pH falls below 4.5. For these reasons, this screening test cannot be recommended [2, 6, 14].
As a result of the poor performance of any one marker for the diagnosis of toxic alcohol ingestion, it is recommended by the American Academy of Clinical Toxicology that the clinician maintain a high index of suspicion and low threshold for treatment [6]. Diagnostic criteria and indications for treatment are shown below [4, 6, 15].
Diagnostic Criteria and Indications for Treatment of Ethylene Glycol Poisoning
Ethylene glycol level >20 mg/dL or
Recent history of known ingestion AND osmolal gap >10 or
Strong suspicion of ethylene glycol ingestion AND two of the following
pH, 7.3
serum bicarbonate <20
osmolal gap >10
Calcium oxalate crystalluria
Ventilator and Circulatory Support
Ethylene glycol exerts effects on GABA and Glutamate receptors in a similar manner to ethanol. In severe poisonings, respiratory depression and/or inability to adequately protect one’s airway may necessitate intubation and mechanical ventilation. When an acidosis is present, attention to adequate minute ventilation is imperative to allow for adequate respiratory compensation.
Hypotension may result from direct vasodilatation caused by the toxic alcohol, or secondary to myocardial depression due to acidosis. In cases of congestive heart failure or impending circulatory collapse, vasopressor agents may be needed. Serial EKGs should be obtained to assess for prolongation of the QTc which may be seen when hypocalcemia is present. Calcium repletion should be limited to patients who are symptomatic (cardiac arrhythmias, seizures), as this may hasten calcium oxalate precipitation in the renal tubules [16]. The presence of hyperkalemia is often the result of extracellular shifts due to the metabolic acidosis, and treatment should be reserved for individuals with concerning EKG manifestations. An ARDS-like picture may rarely develop and should be managed with lung-protective ventilation.
Gastric Decontamination/Lavage/Charcoal
Gastrointestinal decontamination and gastric lavage have limited benefit following ethylene glycol absorption due to its very rapid absorption. Furthermore, toxic alcohols bind poorly to activated charcoal, and its use is not recommended [16].
Aldehyde Dehydrogenase (ADH) Blockade
Inhibition of ADH is the mainstay of treatment and prevents metabolism of ethylene glycol into its toxic metabolites, and it is generally accepted that treatment should be initiated for serum ethylene glycol concentrations in excess of 20 mg/dL [6]. The parent alcohol is then excreted largely unchanged in the urine. The elimination half-life of ethylene glycol ranges from 14 to 20 h in the setting of ADH inhibition [4, 6, 10]. The two ADH inhibitors that may be used are ethanol and fomepizole.
Prior to the advent of fomepizole, ethanol was historically used for ADH blockade. Ethanol is the natural substrate for ADH, and given its higher binding affinity over ethylene glycol, it serves as a competitive inhibitor to toxic alcohol metabolism. The generally accepted regimen for ethanol administration is a loading dose of 600 mg/kg of a 10 % solution IV through a central venous catheter, followed by a continuous infusion of 110 mg/kg/h. The drip is then titrated with a goal serum ethanol concentration between 100 and 125 mg/dL [6, 17]. This requires close monitoring, given the unpredictable pharmacokinetics of ethanol metabolism. Ethanol administration is not without side effects, and patients must be monitored for deterioration of mental status, hypoglycemia, hepatitis, and pancreatitis. When no IV ethanol formulation is available, PO ethanol can be considered using the same serum concentration goal.
Fomepizole (4-methylpyrazole, Antizole) was FDA approved in 1997 for use as a competitive inhibitor of ADH in the setting of toxic alcohol ingestions. Its efficacy was supported through a small prospective clinical sub-study of the Methylpyrazole for Toxic Alcohols (META) trial. Patients treated with fomepizole who had normal renal function at the time of treatment initiation had no subsequent kidney injury. It should be noted, however, that patients with serum ethylene glycol levels exceeding 50 mg/dL also underwent hemodialysis [13]. Fomepizole, when compared to ethanol, has the advantage of predictable pharmacokinetics. Its use is generally well-tolerated although patients occasionally report side-effects including headaches, nausea, and dizziness [13, 18]. A loading dose of 15 mg/kg IV is initiated, followed by 10 mg/kg every 12 h. Fomepizole may induce its own metabolism via the CYP450 pathway, and dosing should be increased to 15 mg/kg every 12 h for doses beyond 48 h of treatment. In patients undergoing concurrent dialysis, the dosing frequency should be increased to every 4 h, or alternatively a continuous infusion of 1 mg/kg/h can be considered [4, 6, 18, 19]. Because ethanol metabolism is inhibited by fomepizole, ethanol treatment should not be used concurrently [20].
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


