Chapter 25 Dealing With Disruptive Behavior in the Perioperative Setting
DEFINING DISRUPTIVE BEHAVIOR
Any action that causes one to feel less than safe is known as disruptive behavior. There are four types of disruptive behavior seen in the workplace. The most common type of disruptive behavior is verbal. Christmas (2007) defined verbal abuse as communication delivered via a behavior, tone, or words that were meant to make an individual feel attacked or humiliated. The words delivered are meant to demean, isolate, belittle, threaten, or accuse a person of an action that is not founded in truth or facts. Psychologic abuse involves aggressive behavior that overtaxes a person’s ability to cope. A bully is one who uses psychologically abusive behavior to control the victim. Bullying is a purposeful exertion of power or intimidation that is physically or emotionally threatening to the victim (Kolanko et al, 2006). In the workforce we are able to identify two types of bullying. Direct bullying includes overt acts of verbal or physical aggression. Indirect bullying involves the use of passive-aggressive behavior or social isolation to intimidate the target. Physical abuse inflicts harm intentionally on another individual. Sexual abuse is accomplished when a person is forced into physical contact that has the sole purpose of humiliating the victim. Disruptive behavior can cross lines of authority and job hierarchy. An example of crossing lines of authority is when a surgeon bullies a certified registered nurse anesthetist (CRNA) and the anesthesiologist gets involved and retaliation occurs (Figure 25-1). The cycle of disruptive behavior is born and will spread quickly throughout the department if not stopped (Figure 25-2). Defining disruptive behavior is the first step toward stopping the behavior in the workplace. The following examples provide insight into what a nurse may experience as a direct result of disruptive behavior and bullying:
• I changed my perception of the entire institution where it happened as a result of the incident.
• I considered the incident to be a major factor in deciding whether or not to leave the institution and work somewhere else entirely.
• My supervisors were unsupportive of me during or after the incident.
• I felt as though I had to give in to the attacker’s demands to avoid disciplinary action from my supervisors.
• I felt as though my professional decisions were being monitored and being called into question after the incident.
• I felt others made subtle “behind the back” negative comments about the incident after it occurred.
• I felt management made me give in and compromise to maintain my status as a satisfactory employee.
• I believe patient care was affected by the incident in a way that could have resulted, or actually did result, in an error or a compromise of patient safety.
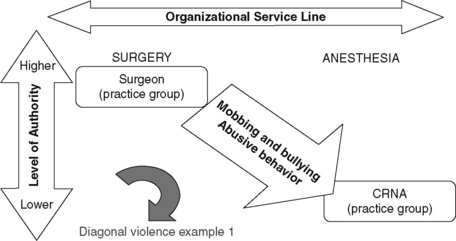
Figure 25-1 Disruptive behavior crossing lines of authority between surgery and anesthesia.
(From Beverly Kirchner, RN, BSN, CNOR, CASC; Jeanie Zelanko, RN, BSN, MSN, PhD; Richard Gilder, RN, BSN, MS.)
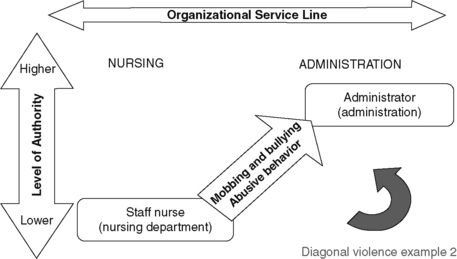
Figure 25-2 Disruptive behavior crossing lines of authority between nursing and administration.
(From Beverly Kirchner, RN, BSN, CNOR, CASC; Jeanie Zelanko, RN, BSN, MSN, PhD; Richard Gilder, RN, BSN, MS.)
Bullying Origins
According to Namie and Namie (2003) 81% of the bullies in the workplace are managers. This is a frightening number in our workplace that can destroy a culture of safety. Every nurse must ask, “What can we do in our workplace to eliminate the bully?” First we have to understand the person and the motivation that causes an individual to define his or her worth by destroying someone else. Where do we first see a bully? The answer is easy; we were first introduced to the bully in school. We noticed the behavior on the playground and in the lunchroom more than in the classroom. Women are far more likely to be bullies than men. The reason is that girls are presumably more likely to get away with passive-aggressive behavior, social isolation of others, and gossip. Young boys tend tobe overt and aggressive in behavior when angry or wanting to control a situation. In contrast, young girls resort to note passing, gossip, and avoidance to isolate another girl who was targeted by the bully. Boys—being overt—get into trouble, whereas girls—passing notes and being passive-aggressive—are not disciplined as often and thus the behavior becomes acceptable.
Bullies in the Workplace
The bully will seek another victim after the target has left the organization. Bullies cannot survive without victims, and victims want nothing to do with bullies. A bully has low self-esteem and uses the target to feel better about his or her behavior. Workplace bullies usually have a lifelong history of disrespecting the needs of others. Namie and Namie (2003) claim that bullies are inadequate, defective, and poorly developed people that destroy others’ self-esteem to feel good about themselves.
CORE ISSUES OF DISRUPTIVE BEHAVIOR
Survey Preparation and Distribution
Every health care facility has to examine the work environment to identify the core issues. The first step toward identifying core issues is to prepare and distribute surveys to physicians and employees (Box 25-1). The survey needs to be designed to explore specific concerns regarding the work environment. Successful data collection depends on ensuring the respondents’ confidentiality. Several concerns that need to be addressed in the survey design include ensuring that the respondents cannot be identified by their description of specific events or handwriting. Using an outside company is one way of providing this guarantee. A facility may be able to work with the information technology department and devise a plan for respondents to answer and feel safe using internal resources. No matter how the plan is designed and implemented, a baseline must be obtained to determine the work environment’s core issues according to the members who work in the environment.
BOX 25-1 Survey Questions to Assess Effects of Bullying
EXAMPLES OF OPEN-ENDED QUESTIONS
1. During the last 6 months of working here, have you changed your perception of this entire institution because of bullying or mobbing (fellow employees and/or supervisors “ganging up” on you)?
2. Do you consider the mobbing-bullying incident you just described above to be a major factor in deciding whether or not to leave the institution and work somewhere else entirely?
3. If you answered yes to any of the previous questions, in your opinion, were your supervisors unsupportive of you during or after the mobbing or bullying incident?
4. During the last 6 months of working here, have you ever felt as though you had to give in to the demands made upon you by those doing the mobbing or bullying to avoid disciplinary action from your supervisors?
Analyzing Responses
The second step in the process involves analysis of the responses received in the survey. It is important to analyze the data and identify key responses to questions, as well as examples of incidents the respondents describe. During the analysis phase the core issues will become apparent and guide the next steps: providing a safe work environment (Box 25-2).
BOX 25-2 Sample Core Issues
• Communication is inappropriate between service X and service Y. The staff in each service line is laying blame on the other team.
• Communication between anesthesiologist A and the nurses is abusive.
• Employees call in frequently when they are scheduled to work with B.
• Employees working in service Z are displaying symptoms of depression.
• The staff working in service W cannot locate a vital instrument when the charge nurse is off (potential sabotage).
Related posts:
 Preventing Surgical Site Infections
Safety in the Perioperative Setting: Vendor Support
Preventing Surgical Site Infections
Safety in the Perioperative Setting: Vendor Support
 To Count or Not to Count: A Surgical Misadventure
To Count or Not to Count: A Surgical Misadventure
 Laser Risks and Preventive Measures for the Staff
Laser Risks and Preventive Measures for the Staff
 Incidence of Deep Venous Thrombosis in the Surgical Patient Population and Prophylactic Measures to Reduce Occurrence
Incidence of Deep Venous Thrombosis in the Surgical Patient Population and Prophylactic Measures to Reduce Occurrence
 Fire Prevention in the Perioperative Setting: Perioperative Fires Can Occur Everywhere
Fire Prevention in the Perioperative Setting: Perioperative Fires Can Occur Everywhere
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


