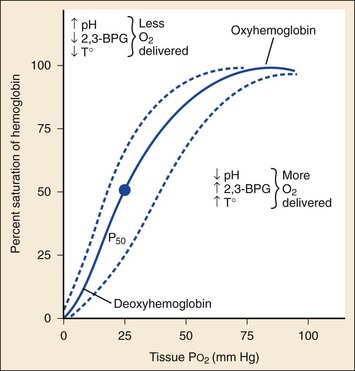
Chapter 14 Cyanosis is evident on physical examination when the absolute amount of desaturated (unoxygenated) hemoglobin in the circulating capillary blood is elevated to approximately 5 g/dL.1,2 It is not a percent of desaturated total hemoglobin mass or a decreased amount of oxyhemoglobin. For this reason, patients with a relatively low hemoglobin level exhibit cyanosis at a much lower partial pressure of oxygen (PaO2) and arterial oxygen saturation (SaO2) than those with normal hemoglobin levels. Cyanosis is an insensitive indicator of tissue oxygenation.3 Its presence suggests hypoxia, buts its absence does not exclude it. Abnormal hemoglobin forms contribute significantly to cyanotic disease. Under normal conditions, red blood cells (RBCs) contain hemoglobin with iron in the reduced ferrous state (Fe2+). The iron molecule may be oxidized to the ferric state (Fe3+) to produce methemoglobin. This reaction impairs the ability of hemoglobin to transport oxygen to and carbon dioxide from the tissues. The oxygen dissociation curve is shifted to the left, resulting in tissue hypoxia and lactic acid production (Fig. 14-1). Methemoglobin normally accounts for less than 1% of total hemoglobin.4 Cyanosis results when greater than 10 to 25% of the total hemoglobin is methemoglobin (approximately 1.5 g/dL), which has a dark purple-brown or chocolate brown color even when exposed to room air. Methemoglobin is reduced to ferrous hemoglobin primarily by nicotinamide adenine dinucleotide (NADH) cytochrome-b5 reductase, an enzyme system present within RBCs. A secondary system dependent on nicotinamide adenine dinucleotide phosphate (NADPH)-reductase uses glutathione production and glucose-6-phosphate dehydrogenase (G6PD) to reduce methemoglobin to hemoglobin. This secondary pathway normally plays a minor role but is accelerated by methylene blue.4 Primary methemoglobinemia is the result of a congenital error in enzyme metabolism, with either diminished levels of NADH reductase or an abnormally functioning enzyme. Patients may have cyanosis in a stable compensated state. Acquired methemoglobinemia occurs when methemoglobin production (hemoglobin oxidation) is accelerated beyond the capacity of NADH reductase activity. This usually occurs as a drug reaction. (See Box 14-1 for common causes.) Newborns are at risk for methemoglobinemia because their NADH reductase activity is relatively low.5 Differential considerations for patients with cyanosis are listed in Box 14-2. BOX 14-2 Differential Diagnosis of Cyanosis A Decreased arterial oxygen saturation 1. Pulmonary arteriovenous fistulae and intrapulmonary shunts 2. Cerebral, hepatic, peripheral arteriovenous fistulae 3. Cyanotic congenital heart disease
Cyanosis
Perspective
Pathophysiology
Diagnostic Approach
< div class='tao-gold-member'>
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree