Fig. 66.1 CXR of our patient
Questions
- 1.
What is the initial prehospital management of a choking child? [1]
- 2.
- 3.
What does the CXR in our patient show?
- 4.
- 5.
Answers
- 1.
Assess severity of choking episode [1].
- (a)
Effective cough (crying or verbal response to questions, loud cough, able to breath before coughing, normal GCS)
Encourage cough—unless patient deteriorates or until obstruction is relieved.
Transport to ED if indicated!
- (b)
Ineffective cough (unable to breath, cyanosis, decreasing GCS, unable to vocalize) [1]
Conscious—blind oropharyngeal finger sweep is not recommended. Alternating five back blows with five chest thrusts (infants) or five abdominal thrusts (child >1 year). Repeat until object comes out or child becomes unconscious.
Unconscious—start CPR.
- (a)
- 2.
History of aspiration from a witness (not always available).
Presentation can range from complete obstruction with hypoxia and cardiac arrest to partial obstruction with symptoms described below to being asymptomatic and presenting later [2].
Symptoms: coughing, choking, stridor or wheezing, drooling, vomiting, chest discomfort, difficulty in swallowing, reduced appetite or refusal to eat, and gagging on eating and drinking.
Signs: tachypnea, intercostal muscles retraction, use of accessory muscles, nasal flaring, or cyanosis.
Sometimes asymptomatic with no physical signs even with a reliable history of aspiration. Sometimes the presentation is with repeated pneumonias or lung abscesses.
Physical examination:
Persistent stridor—high-pitched inspiratory stridor usually a result of supraglottic obstruction.
Biphasic stridor: indicates an obstruction at glottic or subglottic region.
Expiratory stridor: indicates a tracheal or bronchial obstruction.
Decreased breath sounds and wheezing can be indicative of an aspirated FB.
X-rays: AP (Antero Posterior) and lateral x-rays of the chest including the neck must be obtained. Inspiratory and expiratory films will help in lateralizing (radiolucent) FB by emphasizing air trapping. Left and right lateral films are used in young, uncooperative children (the side with the FB will not deflate when placed dependent). Over 50% of X-rays are normal within 24 hours of aspiration.
Radiopaque FB:
It is important to distinguish between a battery/magnet and simple coin. Battery will have a double halo on X-ray and should be removed as a matter of urgency if stuck in the esophagus [5].

Fig. 66.2 FB (ring) at level of thoracic inlet
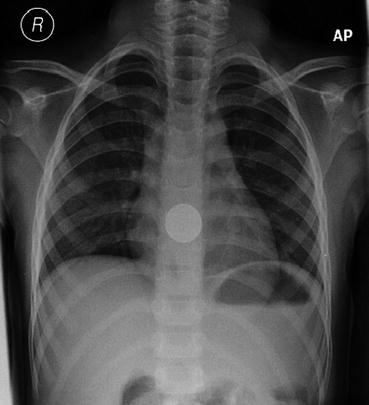
Fig. 66.3 FB (coin) in mid esophagus
Radiolucent FB:Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree




