Fig. 49.1
CT head images of a patient following motor vehicle collision
Questions
- 1.
Define Glasgow Coma Scale.
- 2.
How do you grade traumatic brain injury?
- 3.
What are the common types of traumatic brain injuries?
- 4.
What are the abnormal findings in the images shown above?
- 5.
What are the usual aspects of medical care of a patient with acute traumatic brain injury?
- 6.
Describe some of the important elements of perioperative anesthetic care in a patient with acute traumatic brain injury.
Answers
- 1.
Teasdale and Jennett [3] first described the Glasgow Coma Scale (GCS) in 1974 as a neurological tool to assess the level of consciousness following head injury. The scale is since widely used by medical professionals worldwide as a reliable and objective way of recording the conscious state of a person for initial as well as subsequent assessments. The scale ranges from a minimum score of 3 (not zero) to a maximum score of 15. As described in Fig. 49.2, GCS has three elements: eye response, verbal response, and motor response.
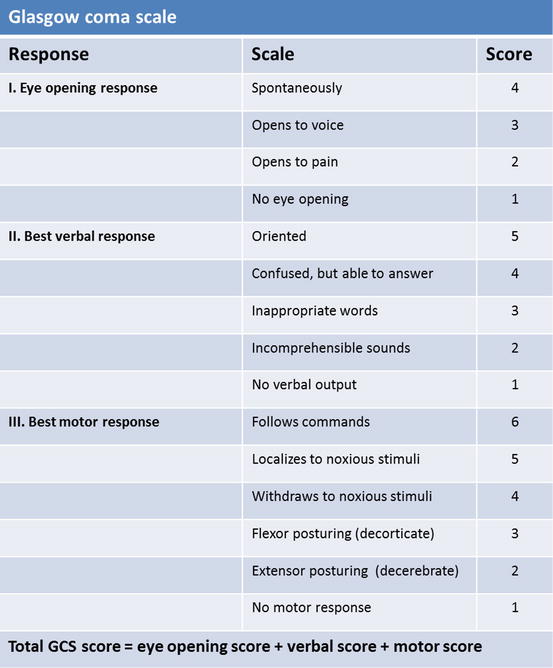
Fig. 49.2
Glasgow Coma Scale
- 2.
Traumatic brain injury (TBI) can be classified as mild, moderate, or severe, based on patient’s Glasgow Coma Scale (GCS) on presentation. A TBI with a GCS of 13 or above is classified as mild, 9–12 as moderate, and 8 or below as severe [4]. The patient described above, therefore, has suffered a severe traumatic brain injury. Other classification systems exist secondary to the limited ability of GCS alone in predicting the outcome. The model developed by the US Department of Defense and Department of Veterans Affairs uses three criteria: GCS after resuscitation, duration of post-traumatic amnesia (PTA), and loss of consciousness (LOC) [5]. It has also been proposed that changes visible on neuroimaging, such as swelling, focal lesions, or diffuse injury, should also be taken into consideration.
- 3.
Some of the common types of traumatic brain injury include epidural hematoma, subdural hematoma, subarachnoid hemorrhage, intraparenchymal hemorrhage, contusion, intraventricular hemorrhage, and diffuse axonal injury. An epidural hematoma is the bleeding from an artery leading to collection of blood between the skull and dura. It can present with the characteristic feature of a lucid interval following which the patient decompensates acutely. It is often a neurosurgical emergency requiring emergent craniotomy and hematoma evacuation. Subdural hematoma is secondary to bleeding from ruptured bridging veins leading to collection of blood between the dura and arachnoid layers of meninges. In elderly, subdural hematomas can occur even from minor trauma and present with symptoms such as new onset headache, seizures, and focal neurological deficits. Subarachnoid hemorrhage is the bleeding into the space between arachnoid membrane and pia mater. Trauma is the leading cause of subarachnoid hemorrhage. Intraparenchymal or intracerebral hemorrhage is the bleeding into the brain tissue itself. A contusion is a small intracerebral hemorrhage commonly noted in orbitofrontal and anterior temporal cortices. Intraventricular hemorrhage is the bleeding into the ventricles of the brain. This is often accompanied by intraparenchymal hemorrhage. An external ventricular drain is usually placed to drain the intraventricular hemorrhage. Diffuse axonal injury (DAI) happens when there is widespread damage to the white matter tracts of the brain secondary to shearing forces. It is one of the most devastating types of traumatic brain injury and can result in persistent vegetative state.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree




