Fig. 48.1
CT showing mediastinal mass causing deviation and crescentic compression of the trachea
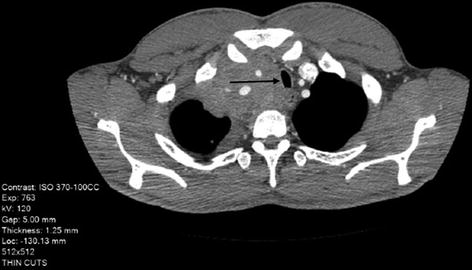
Fig. 48.2
CT showing mediastinal mass posttreatment with less deviation and loss of crescentic compression
A 58-year-old man with a diagnosis of Hodgkin’s disease presents to the anesthesia preoperative clinic prior to placement of a port. He complains of mild difficulty in sleeping totally supine and clinically shows fullness of the veins of the neck. CT scan (Fig. 48.1) shows that he has a mediastinal mass with both tracheal deviation and crescentic compression.
- 1.
What are the symptoms of a mediastinal mass?
- 2.
What are the physical ramifications of a significant mediastinal mass on the airway?
- 3.
What are the anesthesia considerations for a significant mediastinal mass?
- 4.
What are techniques for the safe administration of an anesthetic for a significant mediastinal mass?
Answers
- 1.
Symptoms of a mediastinal mass:
- (a)
A mediastinal mass may be asymptomatic even when it reaches a significant size. It may be discovered during routine radiological testing for the disease causing the mass or just incidentally [1].
- (b)
When the mass reaches a critical size within the restricted mediastinal space, it can cause signs and symptoms related primarily to the cardiac or pulmonary system. This can include diminished venous return via the superior vena cava (SVC) leading to fullness of the neck veins and in extreme cases cardiac dysfunction from direct compression. Respiratory symptoms could range from dyspnea, progressive orthopnea, voice changes (nerve palsy), and in late stages stridor.
- (a)
- 2.
Physical ramifications of the mediastinal mass on the intrathoracic airway:
- (a)
Deviation of the trachea. This could include:
“C”-shaped bowing of the trachea
“S”-shaped trachea
- (b)
Narrowing and invasion of the lumen of the trachea and/or major bronchus:
The trachea when externally compressed becomes crescentic as the membranous posterior wall is the first to collapse.
Narrowing can be a short segment or a long segment of the trachea.
Encroachment can be around the entire carinal trifurcation of the trachea.
- (a)
- 3.
Get Clinical Tree app for offline access
Anesthesia considerations for a significant mediastinal mass:
- (a)
Lack of symptoms should not be considered as reassuring. This is especially true with superior or anterior mediastinal masses. With spontaneous ventilation, the mechanics of thoracic cage cause a distracting force on the larger airways by maintaining the intrapleural pressure gradient, helping to maintain the patency of the lumen. The loss of bronchial tone due to general anesthesia can also decrease lumen size. Thirdly, the distension of the major airways will be diminished with smaller ventilatory volumes [2]. The loss of normal spontaneous ventilation during general anesthesia can thus precipitate intrathoracic airway obstruction in such cases with catastrophic results [3].Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



- (a)


