Chapter 96
Critical Care for the Orthopedic Patient 
Approach to the Patient with Multiple Orthopedic Injuries
All trauma patients should be first evaluated and treated in accordance with the Advanced Trauma Life Support (ATLS) protocol outlined by the American College of Surgeons (see Chapter 95). Of note, patients with fractures of the acetabulum, pelvis, or femur may require a large resuscitation upon presentation. Following the initial resuscitation, all patients should undergo a secondary survey of all organ systems, including the musculoskeletal system. The musculoskeletal survey consists of a head-to-toe, systematic examination that begins with observation. The long bones, axial skeleton (spine, clavicle, pelvis), and joints should be palpated with adequate assessment and documentation of neurologic and vascular function. Range of motion of all major joints should be assessed to detect instability or limitations of motion. In addition, the presence of swelling, ecchymosis, crepitus, visible deformity, and pain will guide further intervention.
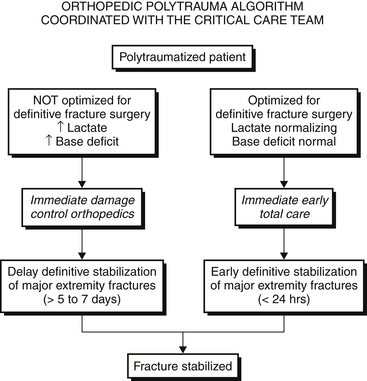
There has been an increased appreciation of the systemic impact that orthopedic injuries have on morbidity and mortality in the polytrauma patient. Much of this work has focused on understanding the outcomes associated with early total care (ETC) versus damage control orthopedics (DCO). The latter appears to be superior and involves the staged management and stabilization of the injuries in order to minimize the complications associated with the “second hit” (physiologic overload after acute trauma as a result of operative interventions) (Figure 96.E1)  . As a result, an increasing number of patients with multiple orthopedic injuries are managed in the ICU for physiologic stabilization prior to definitive management. In contrast to thoracic and abdominal trauma, few orthopedic injuries require immediate surgical management before medical stabilization and optimization. Although not always visible, the energy that is required to induce a fracture can also significantly injure the surrounding tissue envelope. Such compromised soft tissue is not favorable for surgical intervention and can lead to sequelae such as infection, necrosis, or amputation. However, even patients who are felt to be too unstable for definitive fixation still require stabilization of their long bone injuries, compression of pelvic ring injuries, and reductions of dislocations despite their physiologic status.
. As a result, an increasing number of patients with multiple orthopedic injuries are managed in the ICU for physiologic stabilization prior to definitive management. In contrast to thoracic and abdominal trauma, few orthopedic injuries require immediate surgical management before medical stabilization and optimization. Although not always visible, the energy that is required to induce a fracture can also significantly injure the surrounding tissue envelope. Such compromised soft tissue is not favorable for surgical intervention and can lead to sequelae such as infection, necrosis, or amputation. However, even patients who are felt to be too unstable for definitive fixation still require stabilization of their long bone injuries, compression of pelvic ring injuries, and reductions of dislocations despite their physiologic status.
Open Fractures
Fractures with soft-tissue injuries allowing the bone to communicate with the environment are termed open fractures. Open fractures are often associated with high-energy mechanisms or penetrating trauma. These fractures have an increased rate of complications due to soft-tissue disruption and colonization of bacterial flora within the wound. In addition to the general strategies utilized for closed fracture care, open fractures are often taken to the OR on an emergent basis to help prevent infection.
Dislocations
When sufficient translational, rotational, or distractive forces are exerted across a joint, the surrounding soft tissues, including ligamentous and tendinous structures, may become compromised. This can result in a dramatic disruption of the articular congruity of the joint, termed traumatic dislocation (Figure 96.E2)  . Dislocations sustained from higher energy mechanisms are more prone to neurovascular injury, avascular necrosis, and posttraumatic arthritis. Such dislocations need to be reduced emergently by the orthopedic surgeon. Patients with unstable dislocations may require splinting or external fixation.
. Dislocations sustained from higher energy mechanisms are more prone to neurovascular injury, avascular necrosis, and posttraumatic arthritis. Such dislocations need to be reduced emergently by the orthopedic surgeon. Patients with unstable dislocations may require splinting or external fixation.

Orthopedic Care and the ICU
Open Fracture Care
Prophylactic antibiotic treatment is guided by the type of open fracture (Table 96.1). Open fracture typing is based on the degree of soft-tissue involvement and the energy of the injury. The degree and type of contamination must also be considered
TABLE 96.1
Gustilo-Anderson Classification of Open Fractures
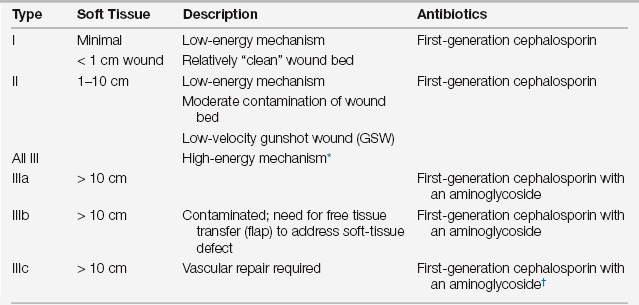
∗Includes segmental fracture, high-velocity GSW, or highly contaminated or crush injury.
†Add penicillin if significant contamination is seen or suspected. Vancomycin or clindamycin may be substituted in the case of penicillin allergy.
Data from Zalavras CG, Patzakis MJ. Open fractures: evaluation and management. J Am Acad Ortho Surg 2003; 11:212-219.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


