11 Uncontrolled haemorrhage has been shown to be the most common cause of preventable deaths in trauma and is responsible for 40% of early in-hospital trauma mortality. Observational studies have shown that 25% of trauma patients also have an established coagulopathy on arrival in the emergency department and that this is associated with a fourfold increase in mortality. The so-called ‘lethal triad of death’ (Figure 11.1) describes the mutually perpetuating combination of acute coagulopathy, hypothermia and metabolic acidosis. These are seen in exsanguinating trauma patients. Hypoperfusion results in reduced oxygen delivery and the consequent switch to anaerobic metabolism results in lactate production and therefore metabolic acidosis. Anaerobic metabolism limits heat production, exacerbating hypothermia caused by exposure to cold resuscitation fluids and blood. It is known that disruption of haemostatic equilibrium occurs at the moment of traumatic impact at which point physiological responses are initiated producing acute traumatic coagulopathy. The degree of coagulopathy has been shown to correlate closely with severity of injury, blood product requirements and mortality. Although the aetiology of acute coagulopathy in trauma is not fully understood, it is thought to involve the disruption of the equilibrium of the clotting cascade:
Control of major haemorrhage
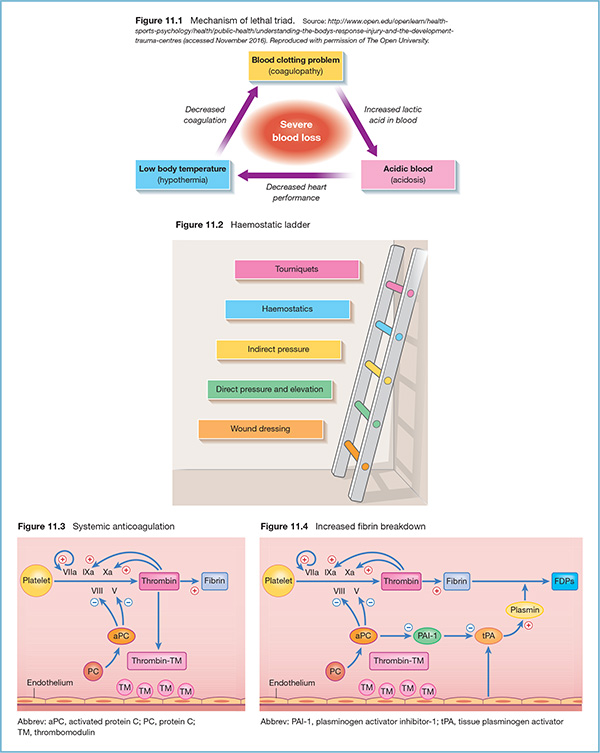
The problem of major haemorrhage in trauma
Acute coagulopathy in trauma
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


