Continuum of Force
Bret T. Ackerman
Jeffrey D. Ho
OBJECTIVES
After reading this section, the reader will be able to:
Describe the types of intermediate weapons available.
Understand the concept of nonlethal weapons and their role in the force continuum.
Understand the potential effects of these weapons on the human body.
Understand the concept of sudden, in-custody death syndrome (ICDS).
INTRODUCTION
The concept of the “force continuum” exists to explain the spectrum of available officer reactions to a subject’s actions. The subject’s actions can range from being completely compliant all the way up to the level of potentially lethal assault. Accordingly, an officer’s perception and reaction to these actions can range from the lowest use of force (generally accepted as “officer presence” without contact to encourage or discourage certain types of behavior) all the way up to the level of deadly force (1). In between these two ends of the spectrum are many options, including empty hand control techniques and the use of intermediate weaponry. There are different models of force continuums used by various law enforcement agencies and each model has inherent advantages and disadvantages. A sample of a federal model is shown and is an example of typical information contained in the continuum, regardless of model type (Fig. 4.1).
Force continuums allow the operator to enter at any level of force deemed reasonably necessary to confront the situation at hand. It is not necessary to escalate from the lowest levels to get to the highest levels if what is needed is a high level of force to meet an officer’s needs. However, it is also not mandatory that the officer stays at a high level of force if the situation calls for a lesser use of force. Essentially, force continuums are designed to be dynamic guides that allow the user to adapt to changing situations.
Within the force continuum lies the use and concept of nonlethal, intermediate weaponry. Intuitively, the term nonlethal leads one to believe that it is any weapon that cannot kill. This is misleading because even benign appearing objects, such as a clipboard or a ballpoint pen, can become lethal weapons given the right circumstances. However, the official definition, as set by the United States military for nonlethal weaponry, is one that is “explicitly designed and primarily employed so as to incapacitate personnel or material, while minimizing fatalities” (2). Certain intermediate weapons available to the modern law enforcement officer fall under the nonlethal category and may include weapons such as conducted electrical weapons, chemical irritants, and impact devices.
Intermediate Weapons
Electrical “stun” type devices are a unique, intermediate style of nonlethal weapon. Also known as conducted electrical weapons (CEWs), electromuscular disruption munitions (EMD) or electronic control devices (ECDs), they are more commonly referred to as a TASER. These weapons are also discussed in Chapter 5.
The most popular CEW in use today is the TASER model X26. It uses compressed nitrogen to fire two metallic darts up to a maximum of 35 feet with a predetermined angled rate of spread. It is capable of transmitting an electrical impulse through two cumulative inches of clothing or air space. When it makes adequate contact and the darts are of adequate separation, it causes involuntary contractions of the regional skeletal muscles which render the subject incapable of voluntary movement. If the darts are fired at very close range and do not achieve adequate separation, full muscular incapacitation may not be achieved and the device is then used to encourage certain behavior through pain compliance. Additionally, the TASER device has electrical contact points at its tip that are approximately
1.5 inches apart. These contact points may be touched to a subject during discharge of the weapon and are also considered a pain compliance technique as the separation is not adequate to cause a full, involuntary contraction of muscles. This technique is often referred to as a “drive stun” mode of operation.
1.5 inches apart. These contact points may be touched to a subject during discharge of the weapon and are also considered a pain compliance technique as the separation is not adequate to cause a full, involuntary contraction of muscles. This technique is often referred to as a “drive stun” mode of operation.
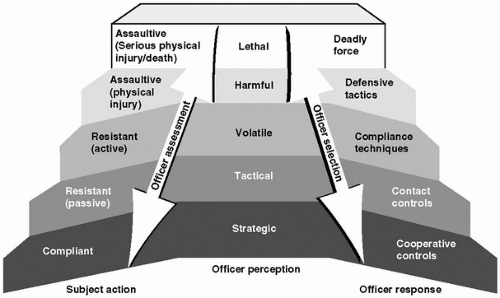 FIGURE 4.1. Sample force continuum. |
It is beyond the scope of this chapter to fully discuss the engineering concepts that allow CEWs to be safe yet effective. Suffice it to say that CEWs utilize high voltage, but very low amperage electrical currents to disrupt normal nerve signals to skeletal muscles. Although this principle of weapon technology has been around for at least 30 years, it has recently improved to the point where it has gained the interest of law enforcement agencies. In doing so, this technology appears to be experiencing the controversial “growing pains” of societal acceptance.
Approximately 15 years ago, chemical irritants, such as pepper spray, were in the same position that TASER devices are today. At that time, chemical irritants entered the law enforcement market and were considered a useful tool for subject control, but critics feared that this new tool would worsen health problems (e.g., asthma) or even cause death (3). Given time, though, this concern was reduced through lab study and observational surveillance. Although chemical irritants were once blamed for in-custody deaths, they are now considered practical and necessary alternatives in use-of-force situations. It appears that CEWs are currently in the throes of a similar acceptance process.
A search of the literature reveals numerous studies, position papers, and review articles about both chemical irritants and CEWs. In fact, the CEW’s continue to be studied by the manufacturer’s, the military, academic institutions, international groups, and law enforcement agencies, making it, arguably, one of the most thoroughly researched piece of equipment found on a law enforcement officer’s duty belt.
Fears of CEW use causing death usually center on theories of electrocution or induced arrhythmia. Because CEWs are more likely to be used on subjects who are actively resisting arrest or in agitated states, there are also theories that they may worsen underlying metabolic acidosis or cause death due to a delayed mechanism, such as induced rhabdomyolysis. These fears are often furthered by media inaccuracies that compare CEWs to electric chairs (4) or civil rights organizations and media stories that may confuse readers by stating conclusions that are not supported by factual data (5, 6 and 7).
There are studies being performed daily on CEW’s and the evidence is mounting against these weapons playing a role in sudden, custodial deaths. Currently, there are studies indicating a high degree of measurable safety margins regarding induction of cardiac arrhythmia, low risk of induced significant myocardial damage when used in typical control settings (the manufacturer of TASER devices reports that the majority of reported uses in the field are for 5-second exposures or less [8]), and no demonstration of induced hyperkalemia or worsening acidosis (9, 10, 11 and 12).
IN-CUSTODY DEATH SYNDROME
Sudden and unexpected in-custody death syndrome (ICDS) is an alarming phenomenon. It leads to suspicion, mistrust, and often inappropriate knee-jerk administrative decisions by involved agencies. The ICDS phenomenon following agitated behavior is not new and similar phenomena have been described in psychiatric literature dating back to the mid-1800s (13). The association with mental illness conditions, especially psychoses with paranoid features, was notable until the mid-1960s when development of traditional antipsychotic medication seemed to correlate with a decrease in these types of deaths (14). In the 1980s, it was noted that there was resurgence in these types of deaths. The rise in these cases has been hypothesized to be related to the introduction and growing popularity of the illicit stimulant cocaine in the street culture of America (15). Currently, we are still experiencing these deaths and they are also being associated with methamphetamine and other illicit stimulant/hallucinogen abuse on an increasing basis.
Over the years, there have been attempts to link ICDS with single causative factors such as use of chemical irritants (e.g., pepper spray), restraint and positional asphyxia, structural cardiac abnormalities, or use of illicit stimulant medication (3,15, 16, 17, 18, 19, 20




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
