Chapter 8 Common problems after ICU
Until recently, an intensive care unit (ICU) stay was deemed successful if a patient survived to go to the ward. No consideration was taken of the patient dying on the ward or soon after leaving hospital or indeed if the patient went home with an appalling quality of life.
Mortality figures for patients leaving our own ICU recently are shown in Figure 8.1.
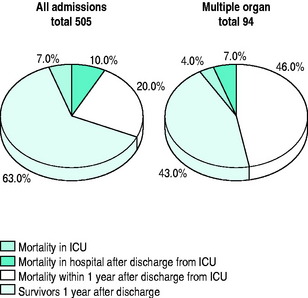
A Kings Fund report1 in 1989 concluded that it was necessary to look at the morbidity following critical illness as well as mortality: ‘There is more to life than measuring death’.
Publications such as that of the Audit Commission (Critical to Success)2 and that of the National Expert Group3 (Comprehensive Critical Care) have supported the development of follow-up for patients following a stay in intensive care. In 2007, the National Institute for Clinical Excellence (NICE) began to take an interest in the rehabilitation of critically ill patients and it is hoped will make recommendations to facilitate the introduction of follow-up programmes in all hospitals looking after critically ill patients.
SETTING UP A FOLLOW-UP SERVICE
The logistics of running the service include arranging specific tests that may be required for the visit, such as pulmonary function tests, swabs for methicillin-resistant Staphylococcus aureus (MRSA), blood/urine for creatinine clearance. There may be special tests such as magnetic resonance imaging (MRI)4 for patients who had a tracheostomy during their stay in ICU.
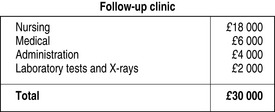
The service in Reading costs £30 000 annually which, in the context of the bigger picture (£4.5 million budget for our ICU), is a small price to pay (Figure 8.2). An unexpected bonus is that the clinic is often seen by the patients as a convenient place to make donations to the ICU.
SPECIFIC PROBLEMS POST-ICU
There are several quality-of-life tools used in follow-up studies (Table 8.1). Objective measurements may be inappropriate because they look at aspects such as return to work: often, patients in their 50s may not return to work after a traumatic episode, including ICU, and subjective measures would be more applicable, such as Perceived Quality Of Life (PQOL).
Table 8.1 Quality-of-life tool examples
| Objective | |
| QALY | Quality of Life tool5 |
| Subjective | |
| HAD | Hospital Anxiety and Depression6 |
| PQOL | Perceived Quality of Life7 |
| EuroQol | ‘European’ tool8 |
| SF 36 | 36-item short-form survey9 |
TRACHEOSTOMY
Since percutaneous techniques performed by intensivists started to replace surgical tracheostomy in 1991, we have seen an increasing number of patients tracheostomised earlier in their ICU stay.
The long-term sequelae have been assessed by lung function tests, nasoendoscopy and MRI screening (Figure 8.3). There are minor cosmetic problems, such as tethering (Figure 8.4). Tethering is easily dealt with in ear, nose and throat outpatients under local anaesthetic.


More difficult to manage is tracheal stenosis, defined as a 15% reduction in tracheal diameter. However, there have only been two cases to date. These were seen in the first series of 30 cases.4
MOBILITY
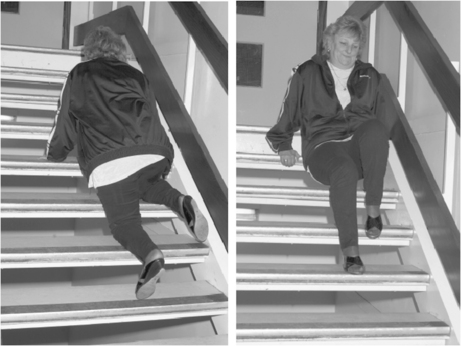
Even in the absence of trauma, patients can expect to need 9 months to 1 year to regain full mobility. This is usually due to a mixture of joint pain, stiffness and muscle weakness. In one study,10 the duration of ICU stay was associated with mobility problems probably associated with loss of muscle mass. If questioned, patients will often report climbing stairs on all fours and descending on their bottoms (Figure 8.5). Muscle wasting can present as a severe localised problem.
This may be associated with critical illness polyneuropathy (CIP),11 which not only prolongs ventilatory weaning but frequently both complicates and delays rehabilitation. Muscle relaxants have been implicated in the development of CIP12 but have not been shown to be statistically significant in terms of delayed weaning of intermittent positive-pressure ventilation and duration of stay in ICU.13
Until now, there have been no specific rehabilitation programmes for patients recovering from critical illness, although rehabilitation programmes for heart attack, stroke and respiratory disease are well established. A three-centre study has shown that a self-help physiotherapy guided rehabilitation exercise programme will speed up physical recovery after intensive care.14
SKIN
Patients complain of a variety of non-specific disorders, including hair loss and nail ridging. Severe pruritus used to be common and not amenable to treatment and was traced back to the use of high-molecular-weight starch solutions in ICU. Described in 2000,15 in 85 cardiac surgical patients, pruritus was absent in the 26 patients who did not receive starch, but there was a 22% incidence in the 59 patients who did receive starch. This is now supposedly less of a problem with the newer starches.
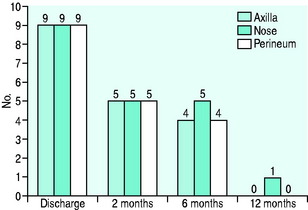
Colonisation with MRSA often persists for up to 9 months or longer (Figure 8.6). It is common to hear that patients are being treated as ‘lepers’ by their own family.
SEXUAL DYSFUNCTION
In a group of 57 patients,16 there was a 39% incidence of sexual dysfunction, although in 4 patients, sex life had improved. Sexual dysfunction improves with time, from a frequency of about 26% at 2 months post-ICU down to 16% at 1 year.17 Sexual dysfunction is often thought to be a psychological problem but, interestingly, following severe burns, it has been reported that there is no correlation between the incidence of posttraumatic stress syndrome and sexual dysfunction.18 Nevertheless, withdrawing sexual intimacy because of fear of failure can damage relationships. Often sexual dysfunction may go untreated because people are too embarrassed to mention the problem when they have recovered from a life-threatening illness.
Sexual dysfunction affects both men and women. In men it usually manifests itself as impotence or inability to maintain an erection sufficient for satisfactory sexual activity. For management guidelines for erectile dysfunction, see Ralph and McNicholas.19
In females, sexual dysfunction may occur due to surgery or trauma to the pelvis. More commonly, there is a reduction in desire. Various lubricating gels can be used. As yet, the role of Viagra for women has to be determined. In 127 patients asked to fill in a questionnaire while attending the clinic, the incidence of sexual dysfunction was 45%.20 There was no link with gender but there was a close association with posttraumatic stress disorder (PTSD).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


