Chapter 69 Chest injuries
CHEST INJURIES
The majority of chest injuries in Australasia result from blunt trauma due to motor vehicle crashes. Less frequent causes include falls and penetrating injuries from stab or gunshot wounds. Associated extrathoracic injuries are common. Chest injuries account for a quarter of all trauma deaths. Immediate death from blunt chest trauma is usually due to blunt rupture of the thoracic aorta, heart or major vessel. Patients who survive the immediate posttrauma period may still have life-threatening injuries that require timely intervention. Most patients can be managed with simple measures, including intercostal tube drainage, analgesia, oxygen therapy and mechanical ventilation. Thoracotomy is infrequently required.1,2
IMMEDIATE MANAGEMENT
During the primary survey a rapid assessment of the respiratory, circulatory and neurological status of the patient is made (Table 69.1). Airway patency is ensured, oxygen administered by facemask and ventilation assessed. Obvious external bleeding is controlled. Two large bore intravenous cannulae are sited, blood samples taken for crossmatch, haematology and biochemistry tests, and intravenous fluids commenced. Intravenous opioid analgesia is given as repeated small boluses, titrated to effect. There are four critical chest injuries that should be sought during the primary survey for which immediate intervention may be life saving:
Table 69.1 Immediate management of chest trauma
In addition, the clinical features of flail chest should be sought as these will no longer be apparent if positive-pressure ventilation is instituted (see below). A chest radiograph is integral to the initial assessment and should be performed promptly. Subcostal ultrasonography of the heart as part of the focused assessment with sonography for trauma (FAST) should be performed with penetrating chest trauma, or if there is haemodynamic instability.3 An ECG is important in the assessment for blunt cardiac injury (see below).4
Endotracheal intubation and mechanical ventilation are indicated for the patient with a compromised airway, severe head injury, or gross hypoventilation and/or hypoxaemia not attributable to pneumothorax. Haemodynamic instability should be anticipated (Table 69.2). Emergency cricothyroidotomy or tracheostomy is only rarely required when an airway obstruction cannot be bypassed by translaryngeal intubation. A nasogastric tube (or orogastric, if facial injuries are suspected) should be inserted to decompress the stomach after endotracheal intubation.
Table 69.2 Causes of cardiovascular collapse on induction of anaesthesia and positive-pressure ventilation in chest-injured patients
PNEUMOTHORAX
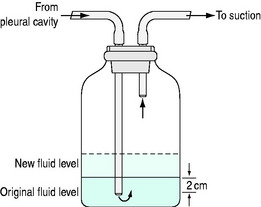
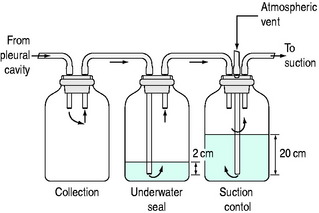
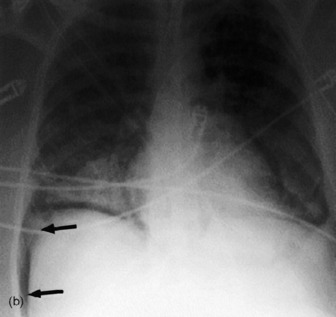
Pneumothorax visible on the initial chest radiograph should be treated with insertion of an intercostal tube connected to an underwater seal drainage system (Figure 69.1). A single-bottle drainage system without suction is usually adequate. Low-pressure suction (20 cmH2O) is applied if the pneumothorax fails to fully resolve, or if there is associated haemothorax (Figure 69.2). A three-bottle system (or commercially available three-in-one system) allows more accurate control of suction (Figure 69.3). Presumptive antibiotics are not indicated.5
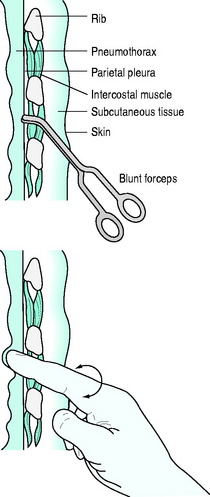
Figure 69.1 Intercostal tube insertion. After sterile preparation and drape, 1% lidocaine is infiltrated in the mid-axillary line at the level of the nipple. A 2–3 cm transverse skin incision is made. Dissection is performed by blunt forceps down to the pleura, passing just superior to the rib surface to avoid injury to neurovascular structures. A gloved finger is used to confirm separation of lung from chest wall. A large bore (32 French) intercostal tube is inserted without a trocar and directed anteriorly for pneumothorax or posteriorly for haemothorax. Curved forceps clamped to the tip of the tube can be used to guide the tube through the chest wall. The tube is immediately connected to an underwater seal drainage system (Figures 69.2 and 69.3) and checked for satisfactory drainage and tidal rise and fall in fluid level with respiration. Non-absorbable sutures are used to seal the skin incision around the tube and secure the tube. The intrathoracic position of the tube is checked with a chest radiograph.
If tension pneumothorax is suspected clinically an intercostal tube should be inserted immediately, prior to the chest radiograph. Needle thoracostomy with a large bore cannula inserted into the second intercostal space in themidclavicular line may be used to drain air more rapidly for patients in extremis. However, this is rarely necessary and may puncture the lung, fail to reach the pleural space, or kink when the needle is removed from within the cannula. Whether successful or not, needle thoracostomy must be followed by formal intercostal tube drainage.
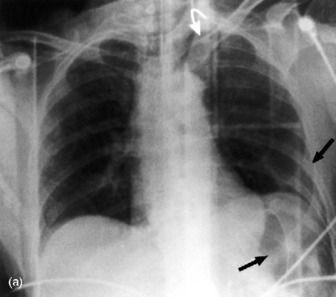
Simple pneumothorax may develop tension at any stage, especially with positive-pressure ventilation (Table 69.2). A small pneumothorax may be missed on the initial chest radiograph. In the supine position pleural air collects anteroinferiorly and is demonstrated radiologically by a deep sulcus sign or increased radiolucency of one side of the chest compared to the other (Figure 69.4).6
Occult pneumothorax is defined as visible on chest CT (or upper slices of an abdominal CT) but not plain radiograph.7 Drainage is not mandatory, but should be considered if prolonged surgery is anticipated, there is significant cardiorespiratory compromise or interhospital transport is necessary. With a conservative approach the patient should be carefully monitored for deterioration from expansion of the pneumothorax.7
Subcutaneous emphysema over the chest wall in a patient with blunt chest trauma is almost always associated with pneumothorax, but should raise suspicion of other injuries (Table 69.3). The pneumothorax may not be visible on the plain chest radiograph, either because it is obscured by the emphysema or because it has largely decompressed into subcutaneous tissues. An intercostal tube should be inserted.
Table 69.3 Causes of pneumothorax, subcutaneous emphysema and/or pneumomediastinum
If there is no associated fluid collection the chest tube can be removed once the pneumothorax is no longer visible on chest radiograph and there has been no air drained for at least 24 hours. Persistent air leak and incomplete drainage of a pneumothorax after intercostal tube insertion should prompt investigation for tracheobronchial injury. However, the depth of the tube within the pleural space and tubing connections should be checked to ensure that extraneous air is not being inadvertently entrained. Incomplete drainage with no air leak is usually due to tube malplacement.
HAEMOTHORAX
Haemothorax visible on chest radiography should be drained as completely as possible (Figure 69.1). The tube can be removed once radiographic clearance is achieved, with < 100 ml/24 hours drainage. A small haemothorax (< 300 ml) (visible on ultrasound or CT) may initially be managed conservatively, but should be drained if it enlarges.
Massive haemothorax, defined as > 1500 ml, causes life-threatening circulatory compromise fromhypovolaemia and vena caval compression as well as hypoxaemia. This requires immediate tube drainage. If the amount of ongoing bleeding following initial drainage is low, the patient remains haemodynamically stable after initial resuscitation, and the blood is venous in appearance, the patient can be managed with close observation. Ongoing bleeding of > 200 ml/h, or > 600 ml over 6 hours (massive haemothorax equivalent), is an indication to proceed to thoracotomy.
PERICARDIAL TAMPONADE
Pericardial tamponade should be suspected in any patient with a gunshot wound to the chest or stab wound to the precordium. It occurs rarely with blunt trauma, but should be suspected if there is hypotension out of proportion to blood loss, and distended neck veins. Pulsus paradoxus may be detected in the spontaneously breathing patient. The differential diagnosis includes tension pneumothorax (most likely) and cardiogenic shock from severe blunt cardiac injury or delayed and inadequate resuscitation. Pericardial fluid can be detected with ultrasound (FAST scan).3 Cardiac structures are imaged via a subcostal view using a low-frequency transducer (3.5 MHz) to provide good tissue depth penetration. Echocardiography, or operative subxiphoid window, can be used if diagnostic uncertainty remains.
Haemodynamically unstable patients should undergo thoracotomy.8 Subxiphoid pericardiotomy can be performed in selected stable patients, but may require conversion to open thoracotomy. Needle pericardiocentesis is rarely effective in the acute setting, but may have a role in the drainage of delayed pericardial effusions following stab wounds.8
CARDIAC ARREST AND EMERGENCY THORACOTOMY
External cardiac massage is invariably unsuccessful in the trauma setting. Indeed, cardiac compression may cause further injury to intrathoracic structures and obstruct access to the patient for more potentially useful interventions such as (bilateral) intercostal tube insertion. For patients with witnessed loss of vital signs after penetrating chest trauma, emergency thoracotomy should be considered if suitably experienced medical personnel are available.8 This is rarely successful for blunt trauma. The standard approach is a left-sided anterolateral thoracotomy. This allows access to the thoracic cavity for specific interventions:8
These temporising (damage control) measures are followed by transfer to the operating room for completion of surgery:9
SPECIFIC INJURIES
Specific chest injuries should be systematically excluded. Imaging techniques play an important role. Choice of investigation is influenced by clinical findings. The degree of haemodynamic and respiratory instability will determine whether the patient can be moved to an imaging facility. Local availability of equipment and clinician expertise may limit the options available. Extrathoracic injuries will often determine investigation and management priorities. With the advent of rapid high-resolution CT scanners, routine chest CT has become increasing popular, particularly in patients who require abdominal or head CT.10 Endotracheal intubation and mechanical ventilation may be required to facilitate investigations (e.g. the combative trauma patient with ethanol intoxication).
BLUNT AORTIC INJURY
Blunt aortic injury usually occurs at the junction between the mobile arch and fixed descending aorta, just distal to the origin of the left subclavian artery, as a result of severe deceleration injury. Less frequently, the ascending aorta or arch vessels are injured by direct trauma. Blunt aortic injuries may be divided into:11
Most patients with blunt aortic injury die at the scene from complete aortic wall transection or associatedinjuries. Of those that reach hospital, 90% will have a significant injury.11 Clinical signs include unequal upper limb pulses, pseudocoarctation or interscapular murmur, but these are rarely detected.12 Aortic injury should be suspected if the mechanism of injury is suggestive of rapid deceleration, such as high speed (greater than 90 km/h) motor vehicle or motorcycle crashes, or a pedestrian hit by a vehicle.13
Historically, chest radiography has been the screening test (to detect mediastinal haematoma) and aortic angiography the diagnostic test for blunt aortic injury.12,14 More recently, CT and echocardiography have been introduced for screening and diagnostic purposes:15


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


