When excessive cerumen causes pain, hearing loss, vertigo, or disequilibrium, it must be removed. Another indication for removal is when it obscures visualization of a symptomatic tympanic membrane.
 Irrigation and manual removal can increase risk of infection in immunocompromised or diabetic patients. Canal trauma can lead to hemorrhage or hematoma in patients on anticoagulants.
Irrigation and manual removal can increase risk of infection in immunocompromised or diabetic patients. Canal trauma can lead to hemorrhage or hematoma in patients on anticoagulants.
 There is no clear evidence in the literature that one method of removing cerumen impaction is superior. There are three options for cerumen removal: (1) cerumenolytic agents, (2) irrigation, and (3) manual removal. These methods may be used alone or in combination. There is no literature support for using cerumenolytics on the first visit and attempting removal with irrigation or manual removal on a second visit.
There is no clear evidence in the literature that one method of removing cerumen impaction is superior. There are three options for cerumen removal: (1) cerumenolytic agents, (2) irrigation, and (3) manual removal. These methods may be used alone or in combination. There is no literature support for using cerumenolytics on the first visit and attempting removal with irrigation or manual removal on a second visit.
 A Cochrane review concluded that no specific cerumenolytic was superior, and none were superior to saline or water, but that most agents led to some clearing of cerumen. Some commercial cerumenolytics can cause side effects, such as local irritation of the canal.
A Cochrane review concluded that no specific cerumenolytic was superior, and none were superior to saline or water, but that most agents led to some clearing of cerumen. Some commercial cerumenolytics can cause side effects, such as local irritation of the canal.
 Procedure for Irrigation
Procedure for Irrigation
 First, explain the procedure to the patient. Ask about the possibility of eardrum perforation or myringotomy tubes, which are contraindications to irrigation. Instill warm (body temperature) water into the canal and let it sit for a few minutes.
First, explain the procedure to the patient. Ask about the possibility of eardrum perforation or myringotomy tubes, which are contraindications to irrigation. Instill warm (body temperature) water into the canal and let it sit for a few minutes.
 Cover the patient with a waterproof drape and have him or her hold a basin or thick towel below the ear.
Cover the patient with a waterproof drape and have him or her hold a basin or thick towel below the ear.
 Fill a 5-mL syringe with body-temperature water, fit it with a short, soft-tubing catheter (Figure 26-1). Aim along the anterosuperior wall of the external canal while pulling the pinna posteriorly to straighten out the canal (do not occlude the whole canal), and squirt quickly to produce a jet lavage. Use a gentler pressure on small children. This irrigation usually needs to be repeated multiple times before the wax is finally flushed out.
Fill a 5-mL syringe with body-temperature water, fit it with a short, soft-tubing catheter (Figure 26-1). Aim along the anterosuperior wall of the external canal while pulling the pinna posteriorly to straighten out the canal (do not occlude the whole canal), and squirt quickly to produce a jet lavage. Use a gentler pressure on small children. This irrigation usually needs to be repeated multiple times before the wax is finally flushed out.
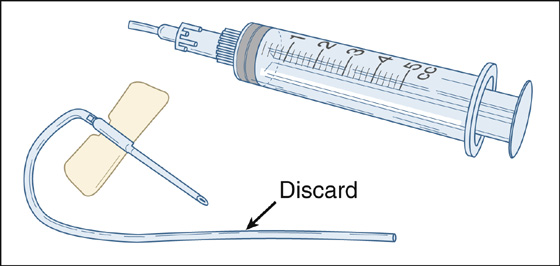
Figure 26-1 Five-mL syringe with short, soft catheter.
 Intermittently reexamine the ear to determine if the wax has been adequately cleared, and if so, grossly test the patient’s hearing. If not, continue irrigating.
Intermittently reexamine the ear to determine if the wax has been adequately cleared, and if so, grossly test the patient’s hearing. If not, continue irrigating.
Procedure for Manual Removal
 If irrigation is contraindicated, unsuccessful, or as an alternative technique, a cerumen spoon (ear curette) may be used. Do not probe blindly into the canal. Perform manual removal under direct vision using an otoscope with the lens removed or using a headlamp. Warn the patient about potential discomfort or minor bleeding before using the curette. Metal curettes are more likely to cause canal trauma.
If irrigation is contraindicated, unsuccessful, or as an alternative technique, a cerumen spoon (ear curette) may be used. Do not probe blindly into the canal. Perform manual removal under direct vision using an otoscope with the lens removed or using a headlamp. Warn the patient about potential discomfort or minor bleeding before using the curette. Metal curettes are more likely to cause canal trauma.
 After irrigation or manual removal, a final rinse with an acetic acid otic solution (Vo Sol Otic) may help prevent secondary otitis. This may be particularly important in older, diabetic, or immunocompromised patients.
After irrigation or manual removal, a final rinse with an acetic acid otic solution (Vo Sol Otic) may help prevent secondary otitis. This may be particularly important in older, diabetic, or immunocompromised patients.
 Finally, warn the patient that he or she may be required to have this procedure done again someday. In addition, warn him or her never to use swabs in the canal, which may increase the risk of future impaction or damage the ear.
Finally, warn the patient that he or she may be required to have this procedure done again someday. In addition, warn him or her never to use swabs in the canal, which may increase the risk of future impaction or damage the ear.
What Not To Do:
 Do not irrigate an ear in which there is suspected or known tympanic membrane perforation or a myringotomy tube.
Do not irrigate an ear in which there is suspected or known tympanic membrane perforation or a myringotomy tube.
 Do not irrigate the ear with cold (or hot) solutions. This may cause severe vertigo with nausea and vomiting. Do not leave pooled water in the canal, which can lead to external otitis.
Do not irrigate the ear with cold (or hot) solutions. This may cause severe vertigo with nausea and vomiting. Do not leave pooled water in the canal, which can lead to external otitis.
This irrigation technique almost always works within 5 to 10 squirts. If the irrigation fluid used is at body temperature, it will soften the cerumen just enough to help it flush out as a plug. If the fluid is too hot or cold, it can produce vertigo, nystagmus, nausea, and vomiting.
A conventional syringe fitted with a large-gauge butterfly catheter (discard any needles) or standard IV extension tubing (J-loop)—either one with its tubing cut 1 cm from the hub—seems to work better than the big, chrome-plated syringes manufactured for irrigating ears. An alternative technique is to use a Water-Pik Oral Irrigator (at the lowest pressure setting).
Metal cerumen spoons or ear curettes can be dangerous and painful, especially for children, for whom this irrigation technique has proven more effective in cleaning the ear canal and allowing assessment of the tympanic membrane. If a cerumen spoon is required, use the soft, disposable, plastic variety.
Cerumen acidifies the ear canal with lysozymes, thereby inhibiting bacterial and fungal growth. It is also hydrophobic and repels water from the ear, further protecting it from infection.
Cerumen is produced by the sebaceous glands of the hair follicles in the outer half of the ear canal, and it naturally flows outward along these hairs. One of the problems associated with ear swabs is that they can push wax inward, away from these hairs, and against the eardrum, where the wax can then stick and harden. Cerumen is most likely to become impacted when it is pushed against the eardrum by these cotton-tipped applicators, hairpins, or other objects that people put down their ear canals, and also by hearing aids. Less common causes of cerumen impaction include overproduction of earwax and an abnormally shaped ear canal.
Advise patients that the best method of cleaning the external ear is to wipe the outer opening of the canal with a washcloth covering the patient’s finger. Instruct them not to enter the ear canal itself.
Patients may ask about “ear candles” to remove wax. Candling, which involves burning a hollow candle inserted into the ear canal, is reported to create a negative pressure within the auditory canal, removing wax and other debris. On the contrary, though, it has been shown that candling does not create negative pressure or remove cerumen and has been found to cause ear injury. It is therefore not recommended.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


