Wendy L. Halm
Bursitis
A bursa is a sac lined with synovial fluid, which provides lubrication and facilitates smooth movement between tissues of an extremity. Bursitis is a pathologic inflammatory disorder of the bursa caused by varied acute or insidious processes. These processes may include trauma or repetitive injury, autoimmune diseases, crystal deposits, and infection.1,2 Bursitis can result in mild pain or become a disabling condition. There are numerous bursae throughout the body, but only a few ever cause problems; these include bursae in the shoulder, hip, knee, elbow, and heel.
A diagnosis of bursitis is usually suspected on clinical grounds. Common features may include pain at motion and at rest; regional loss of range of motion; visible local swelling, especially if the affected bursa lies close to the surface; erythema and warmth over site; and tenderness to palpation.
Shoulder Bursitis
Definition and Epidemiology
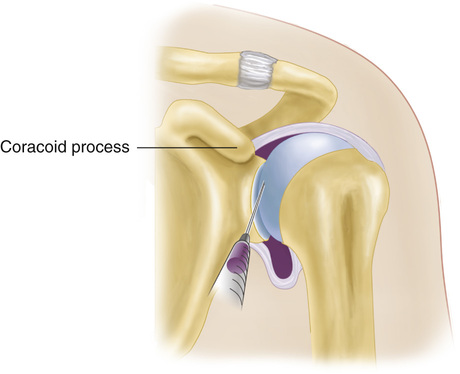
The four major bursae around the shoulder are the subacromial (subdeltoid), subcoracoid, subscapular, and scapular bursae. The subacromial bursa is located between the deltoid muscle and rotator cuff and extends under the acromion and coracoacromial arch. Subacromial bursitis is the most common type of bursitis.1,3 The overhead athlete is at risk for shoulder injury because of the mechanics associated with rapid shoulder elevation, abduction, and external rotation. If it is left untreated, the condition can progress to an irreversible impingement condition.4
Clinical Presentation and Physical Examination
Anterior or lateral shoulder pain with acute or insidious onset is the most common presenting complaint of patients with shoulder bursitis (see Chapter 187). The pain is exacerbated by overhead activities, and there may be a deep aching that interrupts sleep at night. Increased pain with active abduction and internal rotation of the arm plus tenderness below the acromion is demonstrated. Weakness can often be established with internal rotation. A complete neuromuscular examination with careful palpation and passive and active range of motion should be performed. In addition, a quick cervical spine examination can help rule out cervical pain with radiculopathy as the cause of the shoulder pain. The Neer and Hawkins impingement signs are the most sensitive and specific for subacromial bursitis. They indicate inflammation of the subacromial bursa and potentially the rotator cuff (Box 173-1).5,6 Clinicians should be aware of significant clinical diversity regarding the sensitivity and specificity of shoulder diagnostic tests.7–9
Diagnostics
Initial diagnostics should include plain radiography to exclude foreign body penetration, presence of arthritis (and to determine its extent), or fracture.5–7
• Plain radiography may demonstrate a hooked acromion, calcification of the supraspinatus tendon, osteopenia of the humerus greater tuberosity, and a distance of less than 5 mm between the acromion and humerus.6,10,11
Other diagnostics may include the following:
• Ultrasonography can be useful in the diagnosis but is operator dependent and more useful for the identification of rotator cuff pathology.12
• Magnetic resonance imaging (MRI) is now considered the gold standard and is widely used.
If the condition is related to an autoimmune or inflammatory process, serologic tests may reveal an elevated erythrocyte sedimentation rate (ESR), rheumatoid factor, or antinuclear antibodies. If a septic cause is suspected, a white blood cell count as well as a Gram stain and culture of the bursa fluid should be obtained.11 If an aseptic condition is the cause of the bursitis, crystals may be observed in the bursa aspirate (Box 173-2).13,14
Box 173-2
Guidelines for Joint and Bursa Aspiration and Injection
Purpose
Bursa aspiration and injection are performed to obtain bursal fluid for evaluation to determine the cause of the inflammation and for drainage of abnormal fluid accumulation to relieve pain. Local anesthetics, such as lidocaine and corticosteroids, may be introduced into the bursa for symptomatic management of inflammation. Subacromial, trochanteric, anserine, and prepatellar bursitis are conditions that improve with local injection of corticosteroids.
Contraindications
Contraindications to aspiration and injection include cellulitis at the injection site, primary coagulopathy or uncontrolled anticoagulant therapy, septic effusion of a bursa or periarticular structure, more than three previous injections at the same site in the previous 12 months or lack of improvement after two prior injections, suspected bacteremia from another site, unstable joints (for corticosteroid injection), tumors, fractures, joint prosthesis, and inaccessible joints.
Patient Education and Consent
Patient education and consent are necessary before the procedure. The risks and benefits of bursa aspiration should be explained. Adverse effects of introducing a needle into the bursa include infection, bleeding, and pain. Potential complications of corticosteroid therapy include postinjection flare (increased pain for 1 or 2 days), arthropathy, tendon rupture, facial flushing, skin atrophy and depigmentation, transient paresis, transient elevations in blood sugar (if steroid is injected), hypersensitivity reaction, pericapsular calcification, and acceleration of cartilage attrition.
Technique
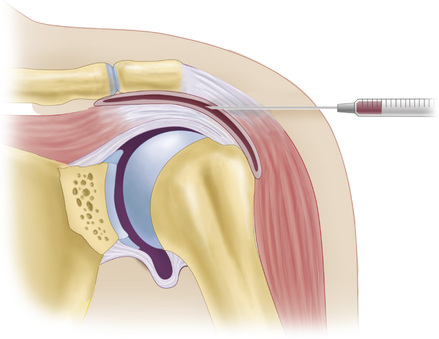
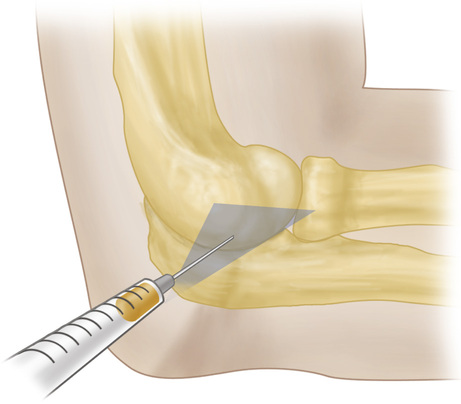
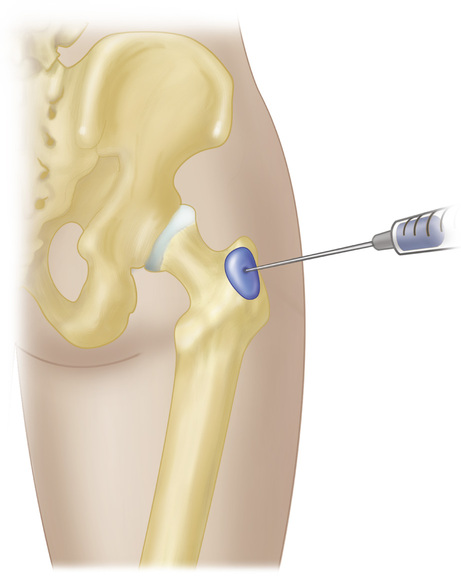
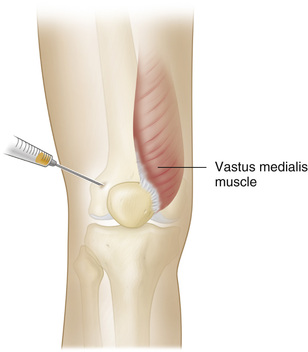
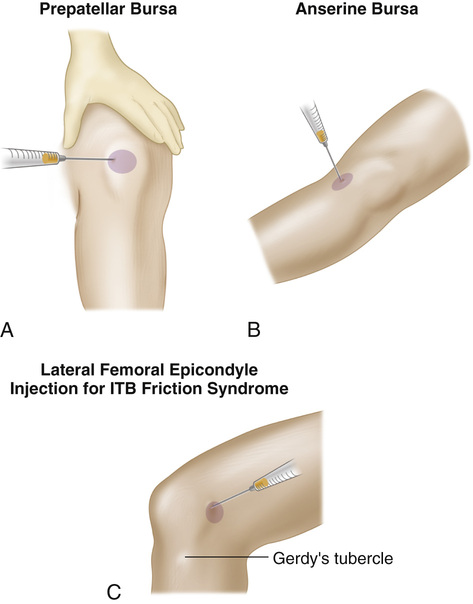
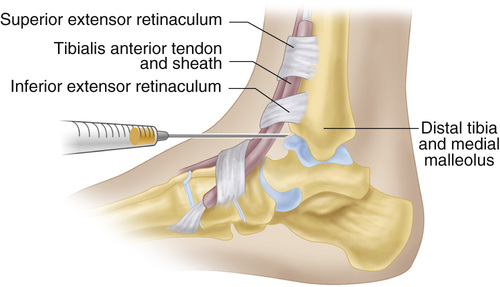
Aseptic technique for bursa aspiration and injection begins by preparing the site for aspiration or injection with povidone-iodine and draping accordingly. The appropriate needle for the procedure is selected: an 18- or 20-gauge needle for aspiration, and a 22- or 25-gauge  -inch needle for injection. A 5- or 10-mL Luer-Lok syringe is recommended. Figures 173-1 to 173-7 demonstrate techniques for aspiration and injection of the more commonly problematic bursae.
-inch needle for injection. A 5- or 10-mL Luer-Lok syringe is recommended. Figures 173-1 to 173-7 demonstrate techniques for aspiration and injection of the more commonly problematic bursae.
A variety of corticosteroid preparations are available in different potencies. The three common corticosteroid local injection therapies for bursitis are hydrocortisone acetate, 25 or 50 mg/mL, which is short acting; triamcinolone acetonide, 40 mg/mL, an intermediate-acting preparation; and long-acting dexamethasone sodium acetate, 8 mg/mL. The typical injected volume will vary from small to large joints.
Lidocaine is combined with the steroid of choice to disperse the steroid at the injection site and reduce procedure-associated pain. A history of lidocaine allergy must first be obtained. Lidocaine, 5 mL, is combined with the steroid for subacromial, trochanteric, or calcaneal bursae. For smaller bursae, such as the olecranon and prepatellar bursa, up to 3 mL of lidocaine combined with the chosen steroid is recommended.
Follow-Up
Procedure aftercare includes applying a bandage over the aspiration-injection site and explaining to the patient that the procedure is provided in addition to other conservative measures and is not a cure in itself. Oral nonsteroidal anti-inflammatory drugs are continued if there is no contraindication. Symptoms of infection should be reported immediately.
Data from Monseau AJ, Singh Nizran P: Common injections in musculoskeletal medicine. Prim Care 40(4):987-100, 2014.
The impingement injection test is one method of differentiating between impingement and other shoulder disorders.3,4 With this test, 10 mL of 1% lidocaine (Xylocaine) is injected into the subacromial space; after 5 to 10 minutes, the maneuvers for the impingement signs are repeated. If the pain is reduced 50%, the shoulder pain is secondary to subacromial bursitis and tendinitis.
Differential Diagnosis
The differential diagnosis includes fracture, dislocation, trauma, arthritis, adhesive capsulitis, rotator cuff tendinitis or tear, muscle strain, and referred pain. Causes of referred pain to the shoulder can include disorders of the cervical spine, chest cavity, breasts, axillary area, and abdomen.6
Management
 Orthopedic specialist referral is indicated for a demonstrated rotator cuff tear, for subacromial fibrosis, to assist in treatment of septic bursitis, or for excision of chronic enlarged bursa when indicated. A rheumatology consultation may be indicated for patients with underlying rheumatoid arthritis who have bursitis.
Orthopedic specialist referral is indicated for a demonstrated rotator cuff tear, for subacromial fibrosis, to assist in treatment of septic bursitis, or for excision of chronic enlarged bursa when indicated. A rheumatology consultation may be indicated for patients with underlying rheumatoid arthritis who have bursitis.
 Immediate emergency department referral is indicated for patients with symptoms consistent with septic bursitis or difficult-to-treat pain. Fever, erythema, warmth, and fluctuance (especially in conjunction with a patient history of diabetes, alcoholism, or impaired skin integrity) should heighten the clinician’s suspicion of septic bursitis.14
Immediate emergency department referral is indicated for patients with symptoms consistent with septic bursitis or difficult-to-treat pain. Fever, erythema, warmth, and fluctuance (especially in conjunction with a patient history of diabetes, alcoholism, or impaired skin integrity) should heighten the clinician’s suspicion of septic bursitis.14
The primary goals of treatment are the reduction of pain and improvement of range of motion. Except for autoimmune and septic shoulder conditions, treatment is directed at rehabilitation of the rotator cuff muscle group. Pain and inflammation may be managed with nonsteroidal anti-inflammatory drugs (NSAIDs) in those without a relative contraindication. During the acute phase, rest and ice may be of benefit. Severe cases of shoulder bursitis may be managed with corticosteroid injections, guided by ultrasound or clinical landmarks. Injections should be limited to three or four injections per 12-month period, no less than 30 days apart.15 Additional therapeutic options may include physical therapy, ultrasound, electrical stimulation, acupuncture, or surgical intervention. Immobilization should be avoided because it may worsen the condition by causing adhesions.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


