• Clinical Considerations
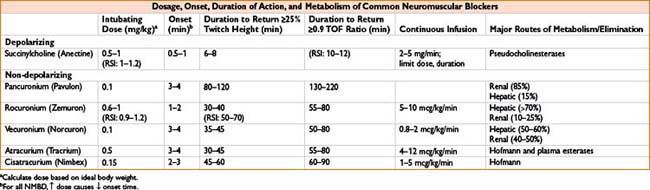
• Indications: Bolus dosing used for rapid sequence induction when aspiration is a risk (i.e., full stomach, trauma, diabetes mellitus, hiatal hernia, obesity, pregnancy); infusion useful in very short surgical procedures requiring relaxation
• Precautions
• Known MH trigger—contraindicated in susceptible patients
• Can ↑ intraocular and intracranial pressure (caution in eye and head injuries), however intubation without adequate relaxation will also ↑ IOP/ICP
• Avoid conditions with extrajunctional ACh receptor proliferation due to potential for ↑↑ potassium release, hyperkalemia (burn pts → probably safe if given <24 hrs or >6 mos of injury; spinal cord transection pts → probably safe if given <24 hrs of injury)
• Limit use in young male patients due to potential for undiagnosed muscular dystrophy and hyperkalemic arrest
• Adverse Effects
• Cardiac: Sinus bradycardia, junctional rhythm, asystole due to stimulation of cardiac muscarinic receptors (especially in patients with ↑ vagal tone, e.g., children). More likely to occur when a second dose of SCh is given within minutes. Pretreatment with atropine may prevent such responses. May also cause tachycardia via ↑ catecholamine release
• Hyperkalemia: Serum K+ transiently ↑ by 0.5–1.0 mEq/L, may be significant in patients with underlying hyperkalemia. As above, ↑↑ K+ release may occur in patients with burns, trauma (especially crush), acidosis, severe infections, prolonged immobility, denervation, stroke, myotonia, muscular dystrophy, and spinal cord injuries
• Allergic reactions: NMBDs are responsible for >50% of the anaphylactic reactions occurring during anesthesia. SCh is the most common cause, followed by rocuronium
• Myalgias: Fasciculation caused by SCh may contribute to postoperative myalgias. Pretreatment with a low dose of a non-depolarizing NMBD (i.e., 1 mg of vecuronium) may decrease the incidence
• Masseter spasm: Sustained contraction of masseter muscle may complicate intubation; can be an early sign of MH though not consistently related (see Appendix C for malignant hyperthermia)
• Increased intragastric pressure: Lower esophageal sphincter tone also ↑, thus no apparent ↑ aspiration risk
ANTAGONISM OF NON-DEPOLARIZING NEUROMUSCULAR BLOCKADE
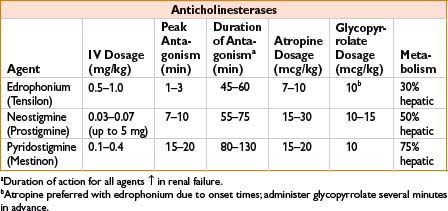
Cholinesterase Inhibitors
• Inhibit acetylcholinesterase, thereby allowing ACh to build up at the NMJ and overcome competitive inhibition non-depolarizers
• Consider relative duration of action of NMBD and reversal agent; administration of reversal after some degree of spontaneous recovery helps prevent “recurarization” (increased weakness in PACU due to lasting effect of NMBD). Note that 70% of ACh receptors may still be blocked with apparently normal TOF
• Common cholinergic side effects of anticholinesterases:
• Cardiac muscarinic effects (bradycardia, sinus arrest). Minimized by concurrent dosing of an anticholinergic drug of similar onset time (glycopyrrolate with neostigmine, atropine with edrophonium; see Chapter 2H-59 for more information on anticholinergics)
• Bronchospasm, ↑ secretions, miosis, nausea, ↑ peristalsis
• Nicotinic effects, especially paradoxical muscle weakness with large doses
• Neostigmine may cross placenta and cause fetal bradycardia, consider concurrent administration of atropine (glycopyrrolate does not cross placenta)
Physostigmine
• Limited usefulness as reversal agent due to penetration of blood–brain barrier; may cause central cholinergic effects (delirium, seizures, impaired consciousness, respiratory depression)
• Used to treat central anticholinergic syndrome (see page 2H-66)
Sugammadex (Proposed Trade Name: Bridion)
• Selective relaxant binding agent—cyclodextrin molecule encapsulates steroid NMBD, rendering it incapable of binding at the NMJ (not currently FDA approved due to hypersensitivity concerns)
• Strongest affinity for rocuronium, may have role in vecuronium and pancuronium reversal as well
• Advantages:
• Can be given at any time after administration of rocuronium, thereby resulting in fast recovery of profound neuromuscular blockade
• Mechanism does not rely on AChE inhibition, therefore no undesirable cardiac effects
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


