![]() Yes or No: Is there intra-abdominal fluid or fluid around the heart?
Yes or No: Is there intra-abdominal fluid or fluid around the heart?
![]() The assessment of blunt thoracoabdominal trauma with significant mechanism of injury
The assessment of blunt thoracoabdominal trauma with significant mechanism of injury
![]() The assessment of penetrating torso trauma if operative management is not immediately indicated
The assessment of penetrating torso trauma if operative management is not immediately indicated
CONTRAINDICATIONS
![]() The FAST examination should never delay a patient’s transport to the operating room when operative management is clearly indicated
The FAST examination should never delay a patient’s transport to the operating room when operative management is clearly indicated
RISKS/CONSENT ISSUES
![]() The only theoretical risk is allergy to the ultrasound gel
The only theoretical risk is allergy to the ultrasound gel
ADVANTAGES
![]() Noninvasive and no sedation required
Noninvasive and no sedation required
![]() Can be performed at the bedside while resuscitative efforts are simultaneously being performed
Can be performed at the bedside while resuscitative efforts are simultaneously being performed
![]() Can be performed at the bedside on patients too unstable for the computed tomographic imaging suite
Can be performed at the bedside on patients too unstable for the computed tomographic imaging suite
![]() Can be repeated serially along with changes in symptoms or hemodynamic stability
Can be repeated serially along with changes in symptoms or hemodynamic stability
LANDMARKS
![]() Subcostal
Subcostal
![]() Probe placed in the subxiphoid region pointed toward the heart detects fluid in pericardial sac
Probe placed in the subxiphoid region pointed toward the heart detects fluid in pericardial sac
![]() Hepatorenal
Hepatorenal
![]() Probe placed in the right midaxillary line between the 8th and 11th ribs detects fluid in the hepatorenal space (Morison pouch)
Probe placed in the right midaxillary line between the 8th and 11th ribs detects fluid in the hepatorenal space (Morison pouch)
![]() Splenorenal
Splenorenal
![]() Probe placed in the left posterior axillary line between the 8th and 11th ribs detects fluid in the splenorenal recess
Probe placed in the left posterior axillary line between the 8th and 11th ribs detects fluid in the splenorenal recess
![]() Suprapubic
Suprapubic
![]() Probe placed 2 cm superior to the symphysis pubis detects fluid in the retrovesical or retrouterine space
Probe placed 2 cm superior to the symphysis pubis detects fluid in the retrovesical or retrouterine space
TECHNIQUE
The standard four FAST views: Subcostal, hepatorenal pouch (Morison), splenorenal, and suprapubic (FIGURE 18.1)
![]() Subcostal/Subxiphoid View (FIGURE 18.2)
Subcostal/Subxiphoid View (FIGURE 18.2)
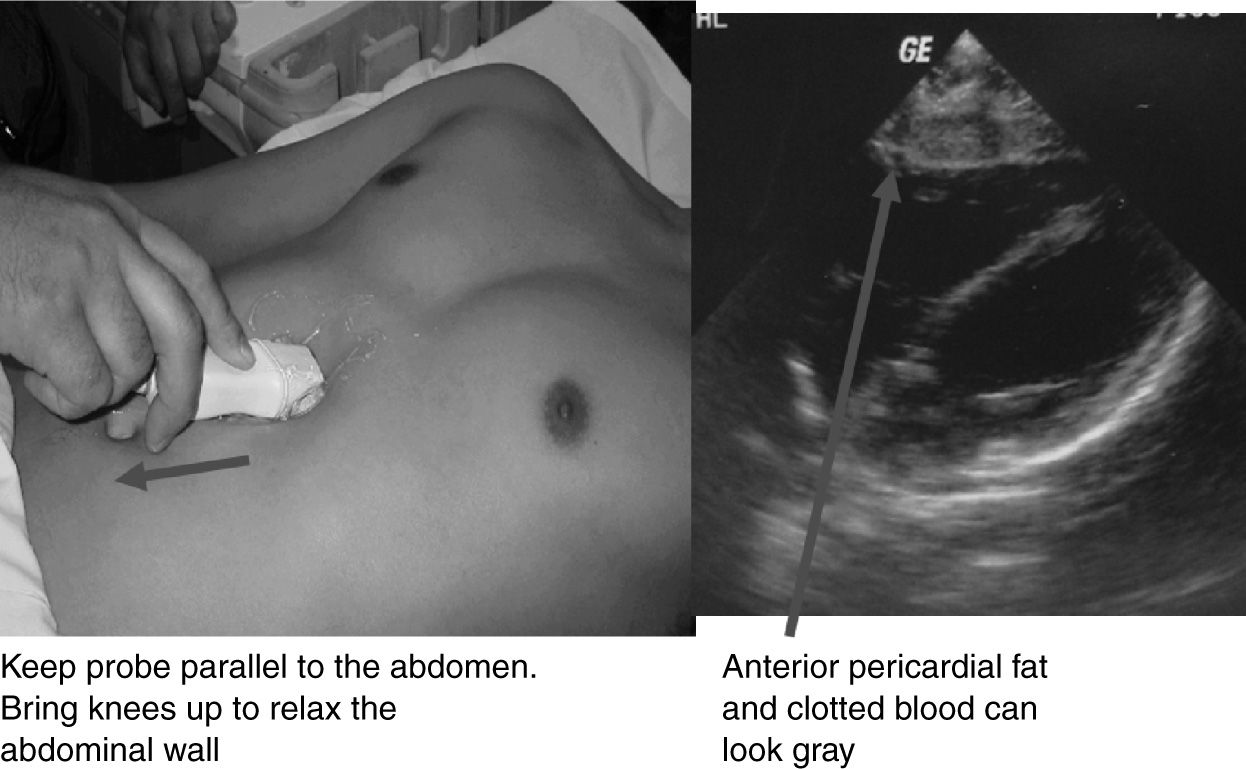
![]() With the probe in the transverse plane, place it in the subxiphoid area and aim toward the patient’s left shoulder to see a four-chambered view of the heart
With the probe in the transverse plane, place it in the subxiphoid area and aim toward the patient’s left shoulder to see a four-chambered view of the heart
![]() Sweep the probe anteriorly and posteriorly to view the entire pericardium
Sweep the probe anteriorly and posteriorly to view the entire pericardium
![]() Unclotted blood will appear as an anechoic black “stripe” within the hyperechoic pericardial sac (FIGURE 18.3)
Unclotted blood will appear as an anechoic black “stripe” within the hyperechoic pericardial sac (FIGURE 18.3)

Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


