![]() Clinical suspicion of abdominal aortic aneurysm (AAA)
Clinical suspicion of abdominal aortic aneurysm (AAA)
![]() Unexplained abdominal, back, or flank pain, particularly in the older patient
Unexplained abdominal, back, or flank pain, particularly in the older patient
![]() Unexplained hypotension
Unexplained hypotension
![]() Syncope in the setting of abdominal pain
Syncope in the setting of abdominal pain
![]() Palpable and/or pulsatile abdominal mass
Palpable and/or pulsatile abdominal mass
CONTRAINDICATIONS
![]() None: No contrast or radiation involved
None: No contrast or radiation involved
LANDMARKS
![]() The proximal aorta is located in the subxiphoid area
The proximal aorta is located in the subxiphoid area
![]() The aorta bifurcates into the iliac vessels at the level of the umbilicus
The aorta bifurcates into the iliac vessels at the level of the umbilicus
![]() On the ultrasound display (FIGURE 12.1), first locate the vertebral body. The transverse proximal aorta is located above (anterior to) the vertebral body, to the right of the inferior vena cava (IVC), and below (posterior to) the superior mesenteric artery
On the ultrasound display (FIGURE 12.1), first locate the vertebral body. The transverse proximal aorta is located above (anterior to) the vertebral body, to the right of the inferior vena cava (IVC), and below (posterior to) the superior mesenteric artery
TECHNIQUE
![]() Apply ultrasond gel on the patient’s abdomen, from the xiphoid process to just distal to the umbilicus
Apply ultrasond gel on the patient’s abdomen, from the xiphoid process to just distal to the umbilicus
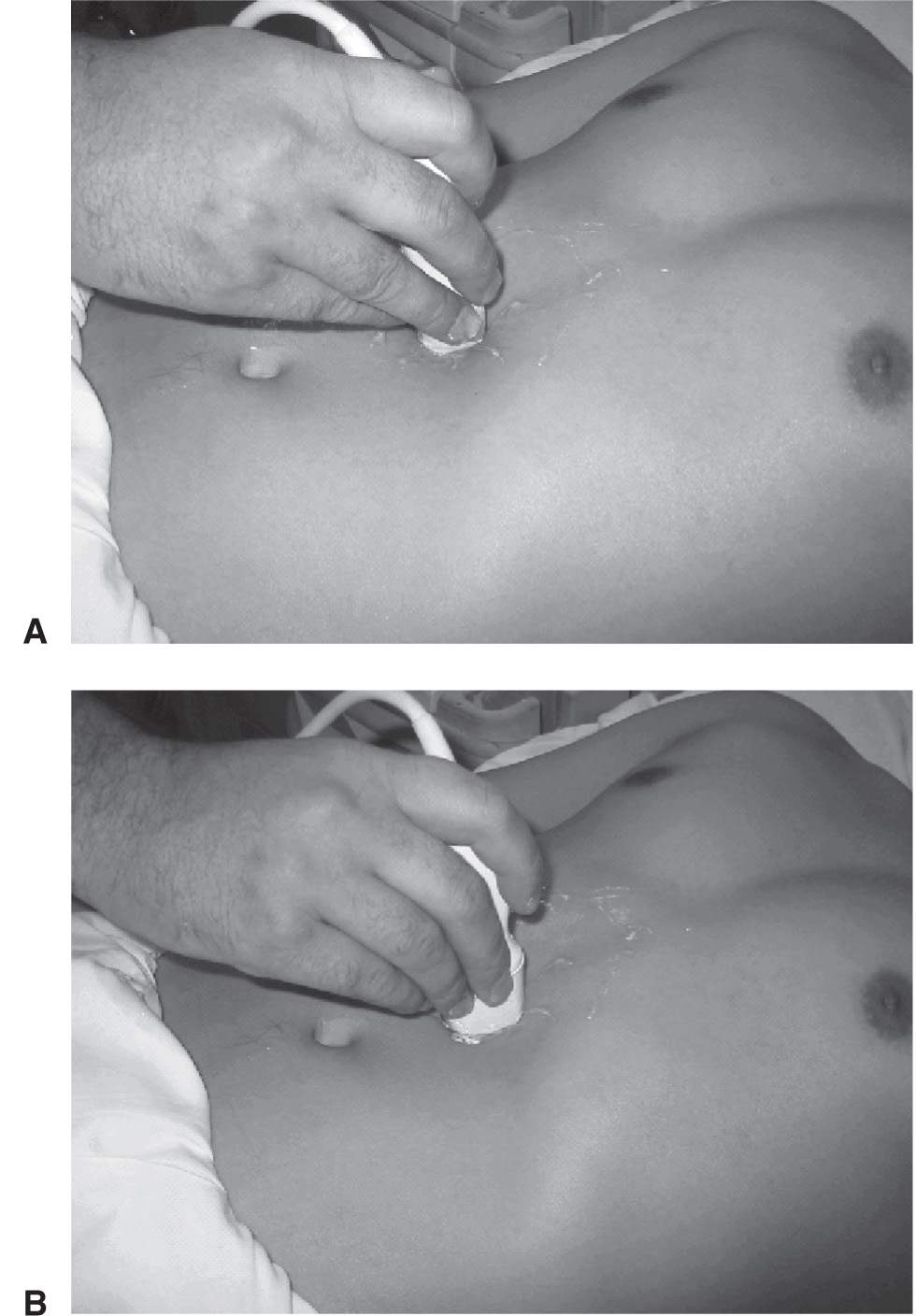
![]() Using a standard 3.5- to 5.0-MHz probe with the selection marker to the patient’s right, identify the proximal aorta in the epigastric area (FIGURE 12.2)
Using a standard 3.5- to 5.0-MHz probe with the selection marker to the patient’s right, identify the proximal aorta in the epigastric area (FIGURE 12.2)
![]() Once the aorta is identified, scan the entire length of the vessel to the iliac bifurcation at the umbilicus
Once the aorta is identified, scan the entire length of the vessel to the iliac bifurcation at the umbilicus
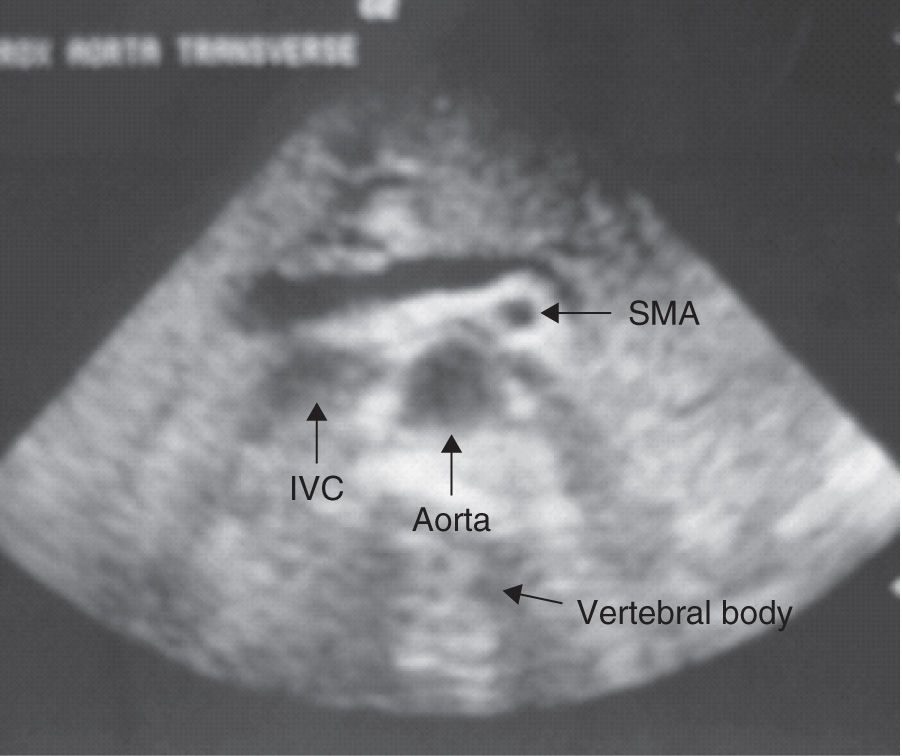
FIGURE 12.1 Transverse proximal aorta anatomy. IVC, inferior vena cava; SMA, superior mesenteric artery. (Courtesy of David Riley, MD.)
![]() Measure the vessel diameter from outer wall to outer wall to avoid underestimation
Measure the vessel diameter from outer wall to outer wall to avoid underestimation
![]() Vessel measurement in the following views permits adequate screening for AAA (FIGURE 12.3):
Vessel measurement in the following views permits adequate screening for AAA (FIGURE 12.3):
![]() Transverse proximal aorta
Transverse proximal aorta
![]() Transverse middle aorta
Transverse middle aorta
![]() Transverse distal aorta
Transverse distal aorta
![]() Transverse view of iliac arteries at the bifurcation
Transverse view of iliac arteries at the bifurcation
![]() Longitudinal aorta
Longitudinal aorta
![]() If an aneurysm is detected (TABLE 12.1), its relation to the renal arteries and aortic bifurcation should be documented if possible (i.e., proximal, distal)
If an aneurysm is detected (TABLE 12.1), its relation to the renal arteries and aortic bifurcation should be documented if possible (i.e., proximal, distal)
![]() If the aorta is not readily identified, try the following techniques:
If the aorta is not readily identified, try the following techniques:
![]() Apply gentle downward pressure with the probe to displace bowel gas
Apply gentle downward pressure with the probe to displace bowel gas
![]() Increase the depth of penetration on the ultrasound display
Increase the depth of penetration on the ultrasound display
![]() Reimaging after several minutes may permit improved visualization as intestinal peristalsis displaces bowel
Reimaging after several minutes may permit improved visualization as intestinal peristalsis displaces bowel
![]() Place the patient in the right or left lateral decubitus position
Place the patient in the right or left lateral decubitus position
![]() Approach para-midline by directing the probe toward the spine to avoid bowel gas
Approach para-midline by directing the probe toward the spine to avoid bowel gas
![]() Image coronally through the liver
Image coronally through the liver
![]() Image inferiorly to the umbilicus and direct the probe cephalad
Image inferiorly to the umbilicus and direct the probe cephalad
COMPLICATIONS
![]() Delay in definitive surgical treatment in order to perform study. Computed tomography (CT) evaluation typically poses a greater time delay.
Delay in definitive surgical treatment in order to perform study. Computed tomography (CT) evaluation typically poses a greater time delay.
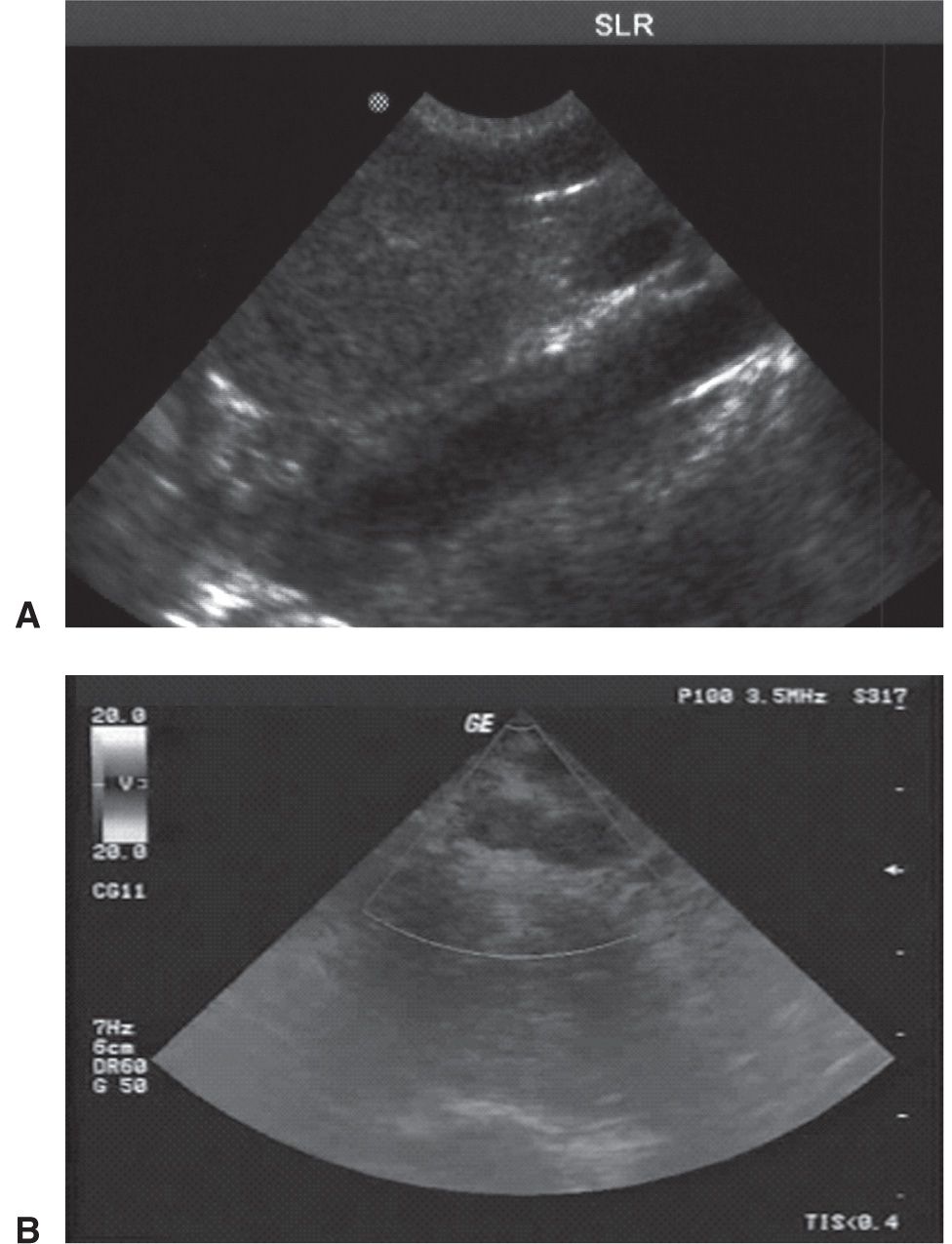
FIGURE 12.3 A: Longitudinal aorta. B: Transverse image of the common iliac bifurcation. (Images courtesy of David Riley, MD.)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


