1 Basic Airway Management
 Key Points
Key Points• Establishment of a patent airway is the cornerstone of successful resuscitation and a defining proficiency of emergency medicine.
• Basic airway management includes the initial airway evaluation and identification and use of interventions to maintain oxygenation and ventilation. These interventions might be simple, such as the application of supplemental oxygen, or complex, such as noninvasive ventilation or emergency tracheal intubation.
• The goal of emergency intubation is safe, successful intubation of the trachea with an endotracheal tube that allows oxygenation and ventilation while protecting the airway from aspiration.
• Patients in the emergency department are always considered high risk because they have not been evaluated beforehand, may have eaten recently, may have anatomic obstacles that are not readily apparent, or may have unstable hemodynamic parameters.
Rapid-sequence intubation (RSI) is the technique of combining sedation and paralysis to create optimal intubating conditions to facilitate emergency intubation. RSI has become the standard in emergency airway management, with intubation success rates greater than 99%.1 The emergency airway operator should fully understand the risks and benefits and also know when to deviate from its standard algorithm.
Airway Assessment
Anatomically, one should assess the patient by looking for facial distortion and the position in which the airway is held. Drooling or inability to tolerate secretions may be apparent and are ominous signs that suggests significant supraglottic irritation. Patients should be asked to open their mouth, or if they are obtunded, a jaw-thrust and mouth-opening maneuver should be performed carefully to determine how far it can be opened. Palpation of facial structures includes determination of nasal, maxillary, and mandibular stability. Maxillary instability, in particular, should alert the practitioner to be cautious with any nasal intubation, whether by nasal trumpet, nasogastric tube, or blind nasotracheal intubation, because intracranial misplacement of nasal trumpets and nasogastric and nasotracheal tubes has been reported.2–6 Once past the facial structures, the tongue should be viewed. Similarly, the hard and soft palate, as well as the tonsils, should be evaluated.
Functional assessment is performed to determine whether the patient can move air and phonate. Specific airway noises should be noted, especially stridor.7 Such assessment leads the clinician to evaluate for specific indications for intubation (Box 1.1).8,9
Oxygenation failure can be defined as an inability to maintain oxygen saturation greater than 90% despite optimal oxygen supplementation (the exception is a patient with chronic obstructive pulmonary failure, who typically maintains a saturation of 85% to 90%).8,10 Ventilatory failure is usually measured by clinical features, including respiratory rate, abnormal depth or work of breathing, abnormal breathing patterns, accessory muscle use, inability to speak in complete sentences, presence of abnormal airway sounds (stridor or severe wheezing), or altered mental status. Studies also point to end-tidal carbon dioxide measurement as an aid in procedural sedation,10 but it is potentially unable to accurately predict PaCO2 in patients with dyspnea.11
Acute obtundation diminishes a patient’s ability to sense irritant stimuli and therefore spontaneously protect the airway.9,12 This is part of the rationale for using a Glasgow Coma Scale score of 8 or lower as a cue to intubate trauma patients.12 Traditionally, the gag reflex has been used to determine whether a patient’s airway reflexes are intact. Stimulation of a gag reflex in an obtunded or trauma patient may result in unwanted patient reactions, however, such as bucking, gagging, coughing, or actual vomiting; additionally, up to 37% of healthy volunteers fail to demonstrate a gag reflex.12,13 Alternatively, a patient who swallows spontaneously while recumbent has sensory and motor paths capable of protecting the airway.12,14,15 In addition, recent articles have questioned use of the Glasgow Coma Scale score in nontrauma patients and instead emphasize clinical judgment in making the decision to intubate.16,17
Critical Airway Physiology
Oxygenation Techniques
The binding of oxygen to hemoglobin is not linear. Hemoglobin tends to bind oxygen well until the partial pressure of oxygen decreases to 60 mm Hg, and then it rapidly dissociates to allow diffusion of oxygen into blood and surrounding tissue. An oxygen partial pressure of 60 mm Hg correlates with an oxygen saturation of approximately 90%18 (Fig. 1.1). This is an important correlation that should be kept in mind throughout resuscitation (Table 1.1).
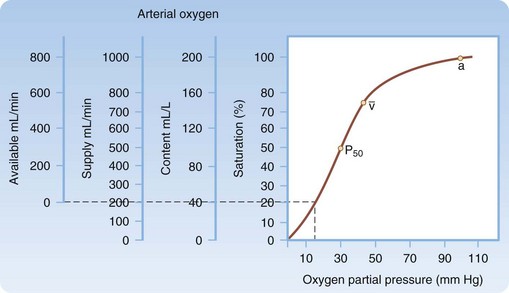
Fig. 1.1 Oxygen-hemoglobin dissociation curve.
 , normal mixed venous pressure; and P50, the partial pressure (27 mm Hg) at which hemoglobin is 50% saturated.
, normal mixed venous pressure; and P50, the partial pressure (27 mm Hg) at which hemoglobin is 50% saturated.(From Miller RD, editor. Miller’s anesthesia. 6th ed. Philadelphia: Churchill Livingstone, 2005.)
Table 1.1 Oxygenation Adjuncts
| DEVICE | RATE | FIO2 (%) |
|---|---|---|
| Nasal cannula | 2 L | 24 |
| Nasal cannula | 4 L | 27 |
| Nasal cannula | 6 L | 30 |
| Venturi mask | — | 40 |
| Nonrebreather mask | 15 L + | 65-70 |
| Bag-mask (one-way inhalation valve + one-way exhalation port, seal maintained without bagging) | 15 L + | 90 |
From Barker TD, Schneider RE. Supplemental oxygenation and bag-mask ventilation. In: Walls RM, Murphy MF, editors. Manual of emergency airway management. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2008. pp. 47-61. Available at http://www.loc.gov.lp.hscl.ufl.edu/catdir/enhancements/fy0807/2007050100-d.html; http://www.loc.gov.lp.hscl.ufl.edu/catdir/enhancements/fy0811/2007050100-t.html.
Patients who require intubation should be preoxygenated with a nonrebreather mask. The goal is to wash as much nitrogen out of the lungs as possible and replace it with oxygen.19–21
When the patient is paralyzed during RSI, this reservoir will permit continued delivery of oxygen to the alveoli for some time, thereby allowing the patient to maintain oxygen saturation while apneic. Five or more minutes of preoxygenation allows this reservoir to develop. Alternatively, if pressed for time, the patient can be asked to take eight vital capacity breaths through the nonrebreather in an attempt to build as great a reservoir as possible.22 Not surprisingly, critically ill patients have decreased oxygen reserve and tolerate apnea less well than do relatively healthy subjects.19,20,23,24
Positive pressure will occasionally be required to oxygenate a patient before intubation. A critical feature of RSI is avoidance of active bag-mask ventilation unless it is absolutely necessary.22 Active bag-mask ventilation with oxygenation is reserved for patients whose oxygen saturation is below 90%.8 Any positive pressure ventilation will not only ventilate the lungs but also insufflate the stomach. This fact is critical to the performance of RSI because a paralyzed patient is at risk for aspiration as a result of relaxed esophageal sphincter tone, especially if the stomach is distended with air.22 Active bag ventilation and oxygenation may need to be performed in patients who are experiencing acute oxygenation failure. Most adult bag-mask devices have reservoirs greater than 1 L and can deliver high-flow oxygen if a good mask seal is maintained.24–26 Alternatively, continuous positive airway pressure or bilevel positive airway pressure can provide a constant level of positive pressure support or two levels of pressure support, respectively, through a tightly fitted mask that fits over the nose or the mouth and nose27,28; if applied in a timely manner in the correct patient, the need for intubation might be averted.
Bag-Mask Technique
Bag-mask oxygenation plus ventilation is a critical skill that all airway managers must master before learning to perform RSI (Boxes 1.2 and 1.3).19 Application of the bag and mask requires proper patient positioning and correct application of a mask seal. The ideal position for mask ventilation is with the patient supine and the head and neck in the sniffing position.19 A proper mask seal is obtained by opposing the mask to the facial skin to create a good air seal. Additionally, new extraglottic devices are available that allow bag ventilation with an inflated balloon surrounding the glottis.29 These devices can also be used to ventilate and oxygenate patients who do not have contraindications (Box 1.4).7,30–37
Box 1.2 Failed Airway Fallback
Mask ventilation is the initial airway management modality of choice for any patient who fails to maintain adequate oxygenation with a nonrebreather mask or begins to desaturate below 90% while apneic during an attempt at rapid-sequence intubation.8
Box 1.4
Causes of Airway Difficulty
Problems with bag ventilation: MOANS (Mask seal, Obesity, Age [>50 years old], Neck mobility, Snores)7,30
Problems with laryngoscopy: LEMON (Look for airway distortion, Evaluate mouth opening and thyromental distance, Mallampati score, Obstruction, Neck mobility)31–37
Problems with cricothyrotomy: SHORT (previous neck Surgery, expanding neck Hematomas, Obesity, previous Radiation therapy, and Tumors and abscesses that might distort the anatomy)7
Problems with the use of extraglottic devices: RODS (Restricted mouth opening, Obstruction, Disrupted or distorted airway, Stiff lungs or cervical spine)36
From Murphy MF, Walls RM. Identification of the difficult and failed airway. In: Walls RW, Murphy WF, editors. Manual of emergency airway management. 3rd ed. Philadelphia: Lippincott, Williams & Wilkins; 2008. pp. 81-93. Available at http://www.loc.gov.lp.hscl.ufl.edu/catdir/enhancements/fy0807/2007050100-d.html; http://www.loc.gov.lp.hscl.ufl.edu/catdir/enhancements/fy0811/2007050100-t.html.
Emergency Airway Algorithm
A patient who merits intubation and is dead or nearly so (a crash airway) requires immediate orotracheal intubation or cricothyrotomy without sedation or paralysis. A patient who is alive and requires intubation will force the airway manager to determine the method of intubation and what medications to use to facilitate it (Fig. 1.2).8
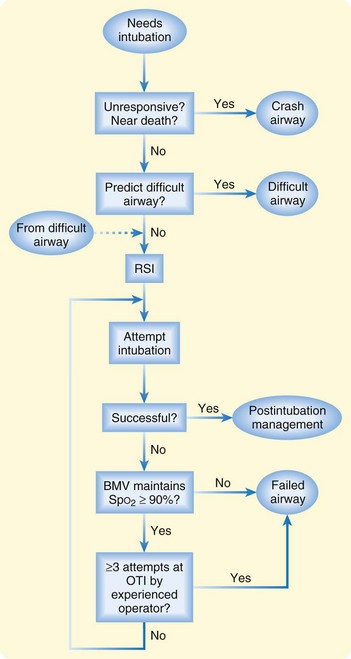
Fig. 1.2 Main emergency airway management algorithm.
(Adapted from Walls RM: The emergency airway algorithms. In Walls RM, Luten RC, Murphy MF, et al, editors. Manual of emergency airway management. 2nd ed. Philadelphia: Lippincott Williams & Wilkins, 2004. Copyright 2004: The Airway Course and Lippincott Williams & Wilkins.)
If the patient is not a crash airway candidate, one should plan to use medications to facilitate intubation. This step requires a determination of expected airway difficulty. Failure to evaluate and anticipate airway difficulty is one of the major causes of failure of intubation.38,39 The use of paralytics in emergency intubation requires preparation for an alternative airway in the event that a patient cannot be intubated by standard means. A difficult airway may preclude the use of paralytics altogether until the clinician can ensure glottic visualization, which is usually obtained with procedural sedation and topical anesthesia. The approach to a difficult airway is discussed in greater detail in Chapter 2.
Unfortunately, there is no universal definition of a difficult airway. Some patients give the clinician an immediate gestalt that their airway will be difficult. Clinicians tend to be correct when their initial reaction is that an airway will be difficult.38,39 The converse is not true. Some otherwise normal-appearing patients will have subtle anatomic differences that may make intubation difficult and are not immediately recognizable by a clinician who is not specifically evaluating for such difficulty.
A number of studies have demonstrated various clinical cues that can be used in an attempt to predict a difficult airway (see Box 1.4). No clinical sign, either alone or in combination with other signs, is 100% sensitive in ruling out a difficult airway.31–35,38,40 However, by using a combination of signs, the vast majority can be identified to make the practitioner aware of potential hazards.
Identification of airway difficulty will require the clinician to give serious thought to performing a sedated examination of the airway with topical anesthesia before proceeding to RSI with neuromuscular blockade (see Chapter 2.)








