CHAPTER 19 Axillary block
Clinical anatomy
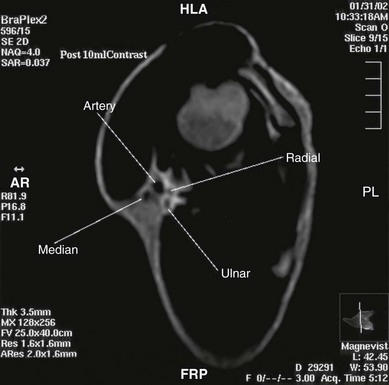
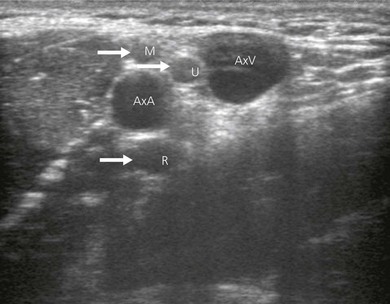
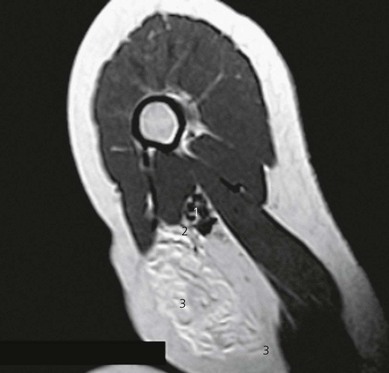
At the site of axillary block the terminal nerves of the brachial plexus form a particular pattern with the axillary artery (Fig. 19.1). Around the second part of the artery – the divisions being produced by the pectoralis minor muscle – the median nerve lies anteriorly, the radial nerve posteriorly, and the ulnar nerve posteromedially (Fig. 19.2). The axillary vein lies more medial. The musculocutaneous nerve has left the fascial sheath at the level of the coracoid and is thus unlikely to be anesthetized with single-injection axillary technique. The medial cutaneous nerve of arm and the intercostobrachial nerve lie subcutaneously.

Sonoanatomy
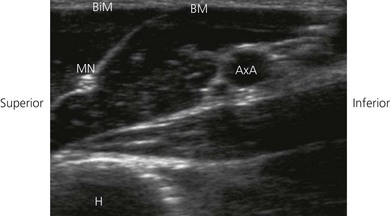
In ultrasound scanning of the axillary brachial plexus, the patient is positioned supine with the arm abducted 90° on an arm board. A linear 6–13 MHz ultrasound transducer is used. Begin the examination by scanning the upper arm in the axilla just distal to the border of the pectoralis muscle. A transverse or short-axis view is used. Perform a systematic anatomical survey from superficial to deep and above and below the axillary artery. Identify the humerus and the triceps, biceps and coracobrachialis muscles. Identify the pulsatile axillary artery. Decrease transducer pressure to allow axillary veins to expand and be identified. The Doppler options facilitate identification of the vascular structures, thereby contributing to minimizing vascular puncture. The nerves lie in a close relationship to the axillary artery near the apex of the axilla, before they start diverging. There is considerable variation in their relationship to the artery and they are very mobile; slight pressure of the transducer can displace the nerves. The nerves appear as hypoechoic structures with a hyperechoic circumference (Fig. 19.3). By sliding the ultrasound transducer proximally towards the apex of the axilla, the musculocutanous nerve can be traced to its origin from the lateral cord (Fig. 19.4). Distally, it diverges from the axillary artery to travel in the coracobrachialis muscle. The axillary nerve also originates from the posterior cord and can be seen going cephalad towards the surgical neck of the humerus. By moving the ultrasound transducer distally, the radial nerve can be traced winding around the humerus.
Technique
Landmark-based approach
The patient lies supine with the arm abducted (80°) and the elbow flexed (90°; Fig. 19.5). Hyperabduction should be avoided because it can make palpation of the artery difficult and distort the distribution of local anesthetic. The axillary artery is palpated as far proximally as possible under the lateral edge of the pectoralis major muscle, and fixed with the index and middle fingers. A 35-mm 21-G insulated stimulating needle is used. The stimulating current is set at 1.0 mA, 2 Hz, and 0.1 ms. The needle is advanced proximally at an angle of 30° in the direction (Fig. 19.6) of the neurovascular sheath. Entry of the needle into the neurovascular sheath is confirmed by a ‘fascial click’. The needle is advanced slowly until the appropriate muscle response is obtained.


Stimulation of the median nerve produces flexion of the middle and index fingers, thumb, and pronation and flexion of the wrist. Stimulation of the ulnar nerve produces flexion of the ring and little fingers with ulnar deviation of the wrist, while stimulation of the radial nerve will produce dorsiflexion of the fingers and wrist. Finger flexion alone in the case of the ring and little fingers could represent either ulnar or median stimulation. The needle position is adjusted while decreasing the current to 0.30 mA with maintenance of the muscle response (Fig. 19.7). A muscle response in the upper arm should not be accepted. Individual nerves can be targeted and located with ease. Ideally, the nerve(s) supplying the area of surgery should be sought.
< div class='tao-gold-member'>






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


