CHAPTER 25 Anterior sciatic block
Surface anatomy
Important bony structures for the anterior landmark-based sciatic block include the anterior superior iliac spine, the pubic tubercle, and the greater trochanter of the femur (Fig. 25.1). A line is drawn between the anterior superior iliac spine and the pubic tubercle (along the inguinal ligament). This line is divided into equal thirds. At the junction between the medial one-third and the lateral two-thirds, a perpendicular line is drawn extending into the thigh. A further line is drawn from the greater trochanter, parallel to the inguinal ligament. Where the perpendicular line crosses this line is the needle insertion point. Rotation of the hip due to leg position or pathology can change anatomic relations; this must be remembered when the needle insertion point is chosen. Important anatomic details include the close proximity of the femoral nerve at the site of needle insertion.

Sonoanatomy
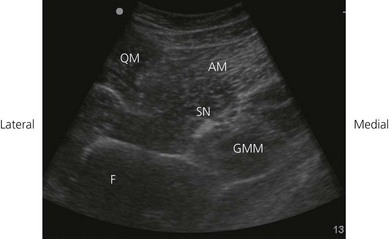
The sciatic nerve may be difficult to visualize in this region because of the required depth of beam penetration and the use of a lower frequency transducer. A transverse transducer orientation is used (Fig. 25.2). Visualization of the sciatic nerve may be obstructed by the lesser trochanter of the femur. Perform a systematic anatomical survey from proximal to distal and from lateral to medial. First identify the femur, a curved hyperechoic line with an underlying bone shadow. Move the transducer proximally and distally to identify the lesser trochanter. Identify the anterior muscular layers: quadriceps muscles laterally and the adductor muscles medially (approximately 8 cm from inguinal crease in adults; Fig. 25.2). Identify the gluteus maximus muscle posteriorly. The gluteus maximus muscle bulk gets smaller as the transducer is moved more distally away from the inguinal crease. Locate the hyperechoic sciatic nerve deep to the adductor muscles and posterior to the femur (Fig. 25.3). The ultrasound image of the sciatic nerve in cross section is typically seen as an oval-to-circular hyperechoic structure. It is often vaguely delineated or appears isoechoic to the surrounding muscles, the latter particularly if using a tangential ultrasound beam plane.

Figure 25.2 Transverse transducer orientation for the ultrasound-guided anterior sciatic nerve block.
< div class='tao-gold-member'>
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


