Pamela Slaven-Lee
Anorectal Complaints
Benign anorectal disorders of structure and/or function include defecatory disorders, fecal incontinence, anal fissure, pruritus ani, proctalgia syndromes, and anorectal abscess and fistula.1 However, other anorectal conditions, such as polyps, condylomata acuminata, malignant neoplasm, and dermatologic disorders, should be considered, because all of these disorders may cause similar symptoms. The correct diagnosis and treatment of any of these disorders require a careful patient history and thorough physical examination. Dietary history should also be obtained because inadequate fiber intake, suboptimal fluid intake, and foods known to alter bowel habits may be revealed as contributory to hemorrhoidal symptoms.2
Hemorrhoids
Definition and Epidemiology
Hemorrhoids are masses of vascular tissue that, along with connective and muscular tissue, form a cushion in the submucosal layer of the anal canal. One of their functions is to help maintain anal closure and continence. They are part of normal human anatomy, and therefore symptomatic hemorrhoids can potentially develop in all adults. External hemorrhoids lie below the dentate line and are covered by squamous epithelium. Internal hemorrhoids are located above the dentate line and are covered by columnar epithelium. Although they are normal anatomic structures, they are infrequently referred to until symptomatic issues arise. Symptomatic hemorrhoidal disease will develop in 50% of the population at some point in their lives, with a peak incidence between the ages of 45 and 65 years. Development of hemorrhoids before the age of 20 is rare,3–5 and pregnancy is associated with a higher risk of symptomatic hemorrhoidal disease.6
Pathophysiology
The exact cause of hemorrhoids is not completely understood. The development of hemorrhoidal disease is most likely multifactorial and influenced by diet, toileting habits, and genetics.2 However, it is thought that submucosal vascular cushions enlarge or prolapse as a result of increased pressure applied to the pelvic floor, causing external or internal hemorrhoids to develop.1,2 Potential causes include pregnancy, straining, lifting, prolonged standing, and irregular bowel habits that contribute to the downward sliding of the vascular cushions in the submucosal layer of the anal canal.2
Clinical Presentation
The most common presenting symptoms of hemorrhoids are bleeding, pruritus, protrusion, and pain. Internal hemorrhoids, which are usually painless, are associated with intermittent, painless, bright red rectal bleeding and intermittent, reducible protrusion that occurs after defecation. The blood may be seen on the toilet paper, in the toilet water, or sometimes on the outside of the stool. Blood mixed in with the stool or dark-colored blood often indicates more proximal disease, whereas bright red blood on the outside of the stool may be suggestive of anorectal pathology.
Internal hemorrhoids can be divided into four categories classified by the degree of prolapse. First-degree hemorrhoids cause bright red, painless bleeding and may bulge but do not prolapse through the anal orifice. Second-degree hemorrhoids prolapse during defecation but reduce spontaneously; patients with second-degree hemorrhoids report bleeding and perineal itching from chronic moisture secreted by the anal canal mucosa. Third-degree hemorrhoids prolapse with defecation and require manual reduction; patients with third-degree hemorrhoids have pain secondary to local ischemia and mucoid drainage.7 Fourth-degree hemorrhoids are permanently prolapsed and are not reducible. It is important to note that the degree of prolapse does not imply incarceration, but nor does prolapse dictate the need for intervention. Hemorrhoidal symptomology and effect on quality of life should guide therapy.1,2 However, incarcerated fourth-degree hemorrhoids require urgent surgical intervention.7 External hemorrhoids are less likely to bleed and are often asymptomatic unless thrombosis develops. The patient can also be seen with anal irritation, pruritus, or a palpable nodule. Symptoms of a thrombosed external hemorrhoid include edema and moderate to severe pain.1
Physical Examination
The entire perineum and perianal area should be inspected with the patient in a comfortable position (knee-chest, lithotomy, or left lateral prone position) while the patient is both at rest and straining.1 External hemorrhoids can be visualized around the anal orifice as the patient bears down, whereas internal hemorrhoids are best visualized with use of an anoscope as the patient bears down. A careful rectal examination is also necessary. An internal hemorrhoid is not palpable on rectal examination unless the hemorrhoid is thrombosed. Inflamed external hemorrhoids are erythematous and sensitive, whereas a thrombosed external hemorrhoid is tender and has a dark, bluish nodular appearance on the anal verge.
Severe rectal pain is unusual but if present suggests a gangrenous or thrombosed hemorrhoid. Gangrenous hemorrhoids are fourth-degree internal hemorrhoids and require immediate surgical evaluation.
Diagnostics
If the history reveals heavy, prolonged bleeding, a complete blood count (CBC) should be obtained to exclude anemia. To screen for bleeding from a more proximal site in the colon, the adult patient should be given stool cards for serial fecal occult blood testing once all hemorrhoidal bleeding has resolved. Any patient who complains of rectal bleeding should undergo endoscopic evaluation to exclude malignant disease. In patients older than age 50 or with a family history of colorectal cancer, the entire colon should be visualized via colonoscopy.1
Differential Diagnosis
The differential diagnosis includes other anorectal conditions that can cause pain, bleeding, or protrusion. Examples are rectal prolapse, anal skin tags, hypertrophied anal papillae, rectal polyps or cancer, anal fissure, anal papillitis, proctitis, inflammatory bowel disease, and condyloma or other sexually transmitted disease.
Management
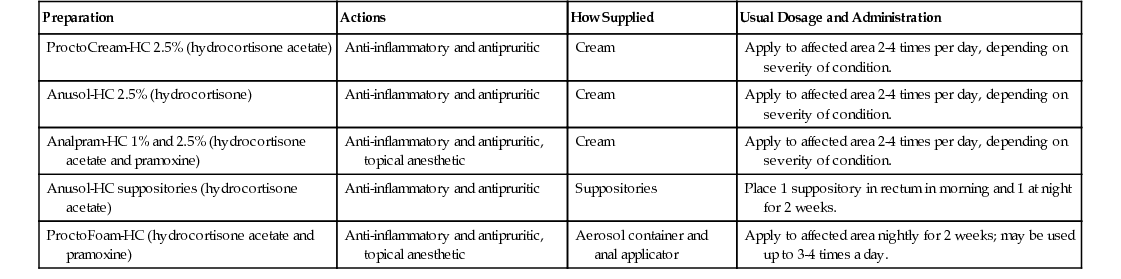
Guidelines for the treatment of benign anorectal disorders such as hemorrhoids were published by the American Gastroenterological Association in 2014.1 The treatment of hemorrhoids is usually based on the degree of the patient’s symptoms and may be categorized as medical management, in-office procedures, and surgical intervention.2 Most hemorrhoids are managed conservatively, and some patients require little or no treatment. A high-fiber diet and increased fluid intake are almost always recommended for the treatment of symptomatic hemorrhoids; according to a Cochrane review, fiber is an effective treatment for symptomatic hemorrhoids, with reduction in hemorrhoidal prolapse and bleeding. Fiber (20 to 30 g/day) absorbs water and helps soften the stool, thus preventing constipation and straining. Bulk-forming agents and stool softeners are sometimes used in addition to diet therapy to keep stools soft. Topical analgesics or hydrocortisone creams and suppositories or foams (Table 128-1), frequent warm water sitz baths, and oral analgesics can help reduce inflammation and promote patient comfort. Laxatives have a limited role in the initial management of hemorrhoids, because the variability in stool consistency associated with chronic laxative use makes hemorrhoid management more difficult.2 Patients with first- to third-degree hemorrhoids that remain symptomatic after diet modification should be referred for in-office procedures such as banding, sclerotherapy, and infrared coagulation.
TABLE 128-1
Topical Anorectal Anti-inflammatory Preparations*
| Preparation | Actions | How Supplied | Usual Dosage and Administration |
| ProctoCream-HC 2.5% (hydrocortisone acetate) | Anti-inflammatory and antipruritic | Cream | Apply to affected area 2-4 times per day, depending on severity of condition. |
| Anusol-HC 2.5% (hydrocortisone) | Anti-inflammatory and antipruritic | Cream | Apply to affected area 2-4 times per day, depending on severity of condition. |
| Analpram-HC 1% and 2.5% (hydrocortisone acetate and pramoxine) | Anti-inflammatory and antipruritic, topical anesthetic | Cream | Apply to affected area 2-4 times per day, depending on severity of condition. |
| Anusol-HC suppositories (hydrocortisone acetate) | Anti-inflammatory and antipruritic | Suppositories | Place 1 suppository in rectum in morning and 1 at night for 2 weeks. |
| ProctoFoam-HC (hydrocortisone acetate and pramoxine) | Anti-inflammatory and antipruritic, topical anesthetic | Aerosol container and anal applicator | Apply to affected area nightly for 2 weeks; may be used up to 3-4 times a day. |
If a thrombosed external hemorrhoid is identified within 3 days of onset, it can be evacuated by first infiltrating a local anesthetic into the base of the hemorrhoid. An elliptical incision is then made into the thrombus, and the clot is expressed. Relief is immediate. This procedure can usually be carried out in the clinic setting by an experienced health care provider but is not indicated in children or in patients who have bleeding disorders, are immunocompromised, or are pregnant. Postoperative care includes a gauze pad applied to the site for 12 hours, followed by a sitz bath to remove the bandage and cleanse the area. Continued daily sitz baths and a minipad to protect clothing are recommended for several more days. If a thrombosed external hemorrhoid has been present for more than 3 days or is not too painful, conservative measures, including mild analgesics, sitz baths, and topical anesthetic ointments, can be used.1,4,7
Researchers continue to investigate newer anesthetic, analgesic, anti-inflammatory, and vasoconstrictive preparations to relieve the discomfort associated with hemorrhoids. In a small study, Rectogesic (glyceryl trinitrate 0.2%) ointment relieved pain, high anal canal resting pressures, and rectal bleeding.8 Phlebotonics, most often composed of natural plant compounds, have proven effective in the management of first- and second-degree hemorrhoids by decreasing vascular endothelial inflammation and normalizing capillary permeability.9
Life Span Considerations
Symptomatic hemorrhoids are a common disease entity. Although they can occur at any age in both sexes, they are more common in adults between 45 and 65 years of age. The prevalence in the United States has been estimated to be as high as 75% of adults older than 50 years.10
Complications
Fourth-degree hemorrhoids are at risk for strangulation because they are irreducible. Strangulated hemorrhoids can become gangrenous, requiring immediate surgical intervention.7
Rubber band ligation has been associated with increased pain, infection, and sepsis. Hemorrhoidectomy has been associated with urinary tract infections, urinary retention, fecal impaction, delayed hemorrhage, and, rarely, infection. Stapled hemorrhoidectomy has been associated with a higher recurrence of hemorrhoids and complications.1,11
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


