Fig.
62.1
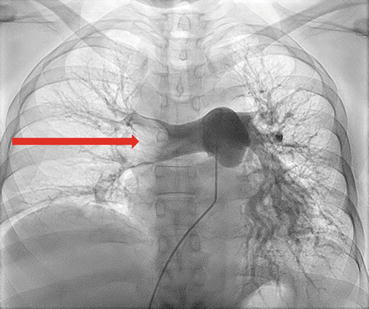
Fig.
62.2
Questions
- 1.
What do these images show?
- 2.
How does one assess the pretest probability for this finding?
- 3.
How does imaging play a role in diagnosis?
- 4.
What are the acute therapeutic options in this situation?
- 5.
When is thrombolytic therapy used?
- 6.
What is the role of catheter based therapy?
Table 62.1
A score of <2 indicates a low probability of pulmonary embolism
Clinical characteristic | Score |
|---|---|
Active cancer | 1 |
Surgery or bedridden for 3 days or more during the past 4 weeks | 1.5 |
History of deep venous thrombosis or pulmonary embolism | 1.5 |
Hemoptysis | 1 |
Heart rate > 100 beats/min | 1.5 |
Pulmonary embolism judged to be the most likely diagnosis | 3 |
Clinical signs and symptoms compatible with deep venous thrombosis | 3 |
- 3.
In patients with high pretest probability for PE, imaging is the test of choice. Pulmonary arteriography is the gold standard for diagnosis of PE. Current generation multi-detector helical computed tomography (CT) has high sensitivity and specificity, comparable to pulmonary arteriography, in detection of PE [2]. Helical CT is the most widely used modality in current clinical settings and would be the diagnostic test of choice in this case. However, in patients with high pretest probability for PE (as in our case) and a negative CT, further investigation in the form of duplex ultrasound of lower extremities or pulmonary arteriography should be considered [3].
- 4.
In patients with high pretest probability for PE, therapeutic anticoagulation should be initiated immediately while awaiting further diagnostic testing (CT, duplex ultrasound, etc.) [4]. Treatment for PE has evolved with the introduction of novel oral anticoagulants or non-warfarin oral anticoagulants (NOAC). Treatment for acute PE can be one of the following:
- (a)
Weight-based low-molecular-weight heparin (LMWH) for 5 days followed by dabigatran, edoxaban, or warfarin (NOACs)
- (b)
Rivaroxaban or apixaban without initial LMWH
- (a)
The treatment for acute PE is divided into the following treatment phases: acute phase of 5–10 days, short-term phase 3–6 months, and long-term phase beyond 6 months. The duration of therapy depends on the underlying cause for the PE and the risk to benefit ratio of anticoagulation.
Outcomes in PE patients depend on the clinical presentation. Based on clinical presentation, they can be further classified into [5]:
- (a)
Massive PE: Acute PE with sustained hypotension (systolic BP < 90 mmHg sustained for over 15 min or requiring ionotropic support) in the absence of any other cause, pulselessness, or profound bradycardia (highest risk of adverse outcomes).
- (b)
Sub-massive PE: Acute PE without sustained hypotension, with signs of hypoperfusion, right ventricular dysfunction on echocardiography, elevated cardiac troponins, and elevated brain natriuretic peptide (intermediate risk of adverse outcomes).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


- (a)


