2 Agitation and Delirium
 Agitation
Agitation
Agitation is a psychomotor disturbance characterized by a marked increase in motor and psychological activity.1 It is a state of extreme arousal, irritability, and motor restlessness that usually results from an internal sense of discomfort or tension and is characterized by repetitive, nonproductive movements that may appear purposeless, although careful observation of the patient sometimes reveals an underlying intent. In the ICU, agitation is frequently related to anxiety or delirium. Agitation may be caused by various factors: metabolic disorders (hypo- and hypernatremia), hyperthermia, hypoxia, hypotension, use of sedative drugs and/or analgesics, sepsis, alcohol withdrawal, and long-term psychoactive drug use to name a few.2,3 It can also be caused by external factors such as noise, discomfort, and pain.4 Associated with a longer length of stay in the ICU and higher costs,2 agitation can be mild, characterized by increased movements and an apparent inability to get comfortable, or it can be severe. Severe agitation can be life threatening, leading to higher rates of self-extubation, self-removal of catheters and medical devices, nosocomial infections,2 hypoxia, barotrauma, and/or hypotension due to patient/ventilator asynchrony. Indeed, recent studies have shown that agitation contributes to ventilator asynchrony, increased oxygen consumption, and increased production of CO2 and lactic acid; these effects can lead to life-threatening respiratory and metabolic acidosis.3
 Delirium
Delirium
Delirium is an acute disturbance of consciousness accompanied by inattention, disorganized thinking, and perceptual disturbances that fluctuates over a short period of time (Figure 2-1).5 Delirium is commonly underdiagnosed in the ICU and has a reported prevalence of 20% to 80%, depending on the severity of illness and the need for mechanical ventilation.6–9 Recent investigations have shown that the presence of delirium is a strong predictor of longer hospital stay, higher costs, and increased risk of death.10–12 Each additional day with delirium increases the risk of dying by 10%.13 Longer periods of delirium are associated with greater degrees of cognitive decline when patients are evaluated after 1 year.12 Thus, delirium can adversely affect the quality of life in survivors of critical illnesses and may serve as an intermediary recognizable step for targeting therapies to prevent poor outcomes in survivors of critical illness.12,14
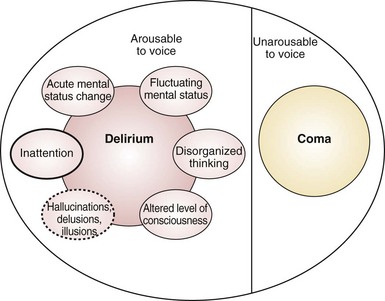
Unfortunately, the true prevalence and magnitude of delirium has been poorly documented because myriad terms—acute confusional state, ICU psychosis, acute brain dysfunction, encephalopathy—have been used to describe this condition.15 Delirium can be classified according to psychomotor behavior into hypoactive delirium or hyperactive delirium. Hypoactive delirium is characterized by decreased physical and mental activity and inattention. In contrast, hyperactive delirium is characterized by combativeness and agitation. Patients with both features have mixed delirium.16–18 Hyperactive delirium puts both patients and caregivers at risk for serious injuries, but fortunately this form of delirium occurs in a minority of critically ill patients.16–18 Hypoactive delirium actually may be associated with a worse prognosis.19,20
Although healthcare professionals realize the importance of recognizing delirium, it frequently goes unrecognized in the ICU.21–28 Even when ICU delirium is recognized, most clinicians consider it an expected event that is often iatrogenic and without consequence,21 though one needs to view this as a form of organic brain dysfunction that has consequences if left undiagnosed and untreated.
Risk Factors for Delirium
The risk factors for agitation and delirium are many and overlap to a large extent (Table 2-1). Fortunately there are several mnemonics that can aid clinicians in recalling the list; two common ones are IWATCHDEATH and DELIRIUM (Table 2-2). In practical terms, the risk factors can be divided into three categories: the acute illness itself, patient factors, and iatrogenic or environmental factors. Importantly, a number of medications that are commonly used in the ICU are associated with the development of agitation and delirium (Box 2-1). A thorough approach to the treatment and support of the acute illness (e.g., controlling sources of sepsis and giving appropriate antibiotics; correcting hypoxia, metabolic disturbances, dehydration, hyperthermia; normalizing sleep/wake cycle), as well as minimizing the iatrogenic factors (e.g., excessive sedation), can reduce the incidence or severity of delirium and its attendant complications.
TABLE 2-1 Risk Factors for Agitation and Delirium
| Age >70 years | BUN/creatinine ratio ≥18 |
| Transfer from a nursing home | Renal failure, creatinine > 2.0 mg/dL |
| History of depression | Liver disease |
| History of dementia, stroke, or epilepsy | CHF |
| Alcohol abuse within past month | Cardiogenic or septic shock |
| Tobacco use | Myocardial infarction |
| Drug overdose or illicit drug use | Infection |
| HIV infection | CNS pathology |
| Psychoactive medications | Urinary retention or fecal impaction |
| Hypo- or hypernatremia | Tube feeding |
| Hypo- or hyperglycemia | Rectal or bladder catheters |
| Hypo- or hyperthyroidism | Physical restraints |
| Hypothermia or fever | Central line catheters |
| Hypertension | Malnutrition or vitamin deficiencies |
| Hypoxia | Procedural complications |
| Acidosis or alkalosis | Visual or hearing impairment |
| Pain | Sleep disruption |
| Fear and anxiety |
BUN, blood urea nitrogen; CHF, congestive heart failure; CNS, central nervous system; HIV, human immunodeficiency virus.
TABLE 2-2 Mnemonic for Risk Factors for Delirium and Agitation
| IWATCHDEATH | DELIRIUM |
|---|---|
| Infection | Drugs |
| Withdrawal | Electrolyte and physiologic abnormalities |
| Acute metabolic | Lack of drugs (withdrawal) |
| Trauma/pain | Infection |
| Central nervous system pathology | Reduced sensory input (blindness, deafness) |
| Hypoxia | Intracranial problems (CVA, meningitis, seizure) |
| Deficiencies (vitamin B12, thiamine) | Urinary retention and fecal impaction |
| Endocrinopathies (thyroid, adrenal) | Myocardial problems (MI, arrhythmia, CHF) |
| Acute vascular (hypertension, shock) | |
| Toxins/drugs | |
| Heavy metals |
CHF, congestive heart failure; CVA, cerebrovascular accident; MI, myocardial infarction.
 Pathophysiology
Pathophysiology
The pathophysiology of delirium is poorly understood, although there are a number of hypotheses:
 Assessment
Assessment
Recently the Society of Critical Care Medicine (SCCM) published guidelines for the use of sedatives and analgesics in the ICU.35 The SCCM recommended routine monitoring of pain, anxiety, and delirium and documentation of responses to therapy for these conditions.
There are many scales available for the assessment of agitation and sedation, including the Ramsay Scale,36 the Riker Sedation-Agitation Scale (SAS),37 the Motor Activity Assessment Scale (MAAS),38 the Richmond Agitation-Sedation Scale (RASS),39 the Adaptation to Intensive Care Environment (ATICE)40 scale, and the Minnesota Sedation Assessment Tool (MSAT).40 Most of these scales have good reliability and validity among adult ICU patients and can be used to set targets for goal-directed sedative administration. The SAS, which scores agitation and sedation using a 7-point system, has excellent inter-rater reliability (kappa = 0.92), and it is highly correlated (r2 = 0.83 to 0.86) with other scales. The RASS (Table 2-3), however, is the only method shown to detect variations in the level of consciousness over time or in response to changes in sedative and analgesic drug use.41 The 10-point RASS scale has discrete criteria to distinguish levels of agitation and sedation. The evaluation of patients consists of a 3-step process. First, the patient is observed to determine whether he or she is alert, restless, or agitated (0 to +4). Second, if the patient is not alert and does not show positive motoric characteristics, the patient’s name is called and the sedation level is scored, depending on the duration of eye contact (−1 to −3). Third, if there is no eye opening with verbal stimulation, the shoulder is shaken or the sternum is rubbed, and the response is noted (−4 or −5). This assessment takes less than 20 seconds and correlates well with other measures of sedation (e.g., Glasgow Coma Scale [GCS], bispectral electroencephalography, neuropsychiatric ratings).39
TABLE 2-3 Richmond Agitation-Sedation Scale
| +4 | Combative | Combative, violent, immediate danger to staff |
| +3 | Very agitated | Pulls or removes tube(s) or catheter(s); aggressive |
| +2 | Agitated | Frequent nonpurposeful movement; fights ventilator |
| +1 | Restless | Anxious, apprehensive, but movements not aggressive or vigorous |
| 0 | Alert and calm | |
| −1 | Drowsy | Not fully alert but has sustained (>10 sec) awakening (eye opening/contact) to voice |
| −2 | Light sedation | Drowsy; briefly (<10 sec) awakens to voice or physical stimulation |
| −3 | Moderate sedation | Movement or eye opening (but no eye contact) to voice |
| −4 | Deep sedation | No response to voice, but movement or eye opening to physical stimulation |
| −5 | Unarousable | No response to voice or physical stimulation |
| Procedure for Assessment | ||
| 1. Observe patient. Is patient alert, restless, or agitated? | (Score 0 to +4) | |
| 2. If not alert, state patient’s name and tell him or her to open eyes and look at speaker. Patient awakens, with sustained eye opening and eye contact. | (Score −1) | |
| Patient awakens, with eye opening and eye contact, but not sustained. | (Score −2) | |
| Patient does not awaken (no eye contact) but has eye opening or movement in response to voice. | (Score −3) | |
| 3. Physically stimulate patient by shaking shoulder and/or rubbing sternum. No response to voice, but response (movement) to physical stimulation. | (Score −4) | |
| 4. No response to voice or physical stimulation | (Score −5) | |
From Sessler CN, Gosnell MS, Grap MJ, et al. The Richmond Agitation-Sedation Scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med 2002;166(10):1338-1344.
Until recently, there was no valid and reliable way to assess delirium in critically ill patients, many of whom are nonverbal owing to sedation or mechanical ventilation. However, a number of tools have been developed recently to aid in the detection of delirium in the ICU. These tools have been validated for use in both intubated and nonintubated patients and measured against a “gold standard,” the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria. The new tools are the Confusion Assessment Method for the ICU (CAM-ICU),42–46 the Intensive Care Delirium Screening Checklist (ICDSC),7 and the Neelon and Champagne (NEECHAM) Confusion Scale.47,48
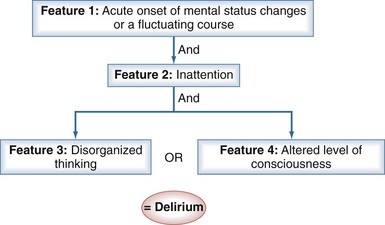
The CAM-ICU (Figure 2-2) is a delirium measurement tool that was developed by a team of specialists in critical care, psychiatry, neurology, and geriatrics.42,49 Administered by a nurse, the evaluation takes only 1 to 2 minutes to conduct and is 98% accurate for detecting delirium as compared with a full DSM-IV assessment by a geriatric psychiatrist.42,43 To perform the CAM-ICU, patients are first evaluated for level of consciousness; patients who respond to verbal commands (a RASS score of −3 or higher level of arousal) can then be assessed for delirium. The CAM-ICU comprises four features: (1) a change in mental status from baseline or a fluctuation in mental status, (2) inattention, (3) disorganized thinking, and (4) altered level of consciousness. Delirium is diagnosed if patients have features 1 and 2, and either 3 or 4 is positive (see Figure 2-2).
< div class='tao-gold-member'>
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


