Chapter 17 Adult cardiopulmonary resuscitation
The incidence and outcomes of cardiac arrests appeared not to have changed dramatically over a number of decades. However, a number of recent advances offer significant promise in our attempts to increase neurologically intact survival.
PREVALENCE AND OUTCOMES OF CARDIAC ARRESTS
Approximately 75% of deaths from cardiac arrests occur in the pre-hospital setting.1 Cardiac arrests in the community occur at approximately 50–150/100 000 person-years.2–4 This incidence (and the outcome) is dramatically affected by the definition of the denominator (e.g. all cardiac arrests (89/100 000 person-years) versus those with a presumed cardiac cause and where resuscitation was attempted (31/100 000 person-years)3).
In-hospital cardiac arrests occur at approximately 1–5/1000 admissions,5,6 with a similar denominator effect (as the majority of in-hospital cardiac deaths are expected and occur without attempts at resuscitation7).
The majority of cardiac arrests in both pre- and in-hospital settings appear to be of cardiac origin, but the underlying causes, comorbidities and presenting rhythms vary significantly between studies.4,6,8,9
Outcomes of cardiac arrests are variable depending on the origin of the report, and are also critically dependent on the denominator.2,3,10 The best outcomes from a cardiac arrest (near 100%) occur in the electrophysiology laboratory (where ventricular fibrillation [VF] is often deliberately induced). The outcomes from in-hospital cardiac arrest are surprisingly good (hospital discharge as high as 42%) despite significant comorbidities, and are probably related to their early detection and the early arrival of the advanced life support (ALS) team.6
INTERNATIONAL REVIEW PROCESS
Since the formation of the International Liaison Committee on Resuscitation in 1992, a cooperative international evaluation of the resuscitation science has resulted in the publication of international guidelines in 200011 and an international consensus on resuscitation science in 2005.12 The published guidelines of the major resuscitation councils throughout the world (including the American Heart Association,13 the Australian Resuscitation Council (www.resus.org.au) and the European Resuscitation Council14) are based on this document. The process for the 2005 consensus on resuscitation science involved the review of 276 topics by 281 international contributors, with the completion of 403 worksheets15 (completed worksheets available at www.c2005.org). This science review process continues to be refined and a new consensus on resuscitation science document is planned for publication in 2010.
IMPORTANCE OF CHAIN OF SURVIVAL
The term ‘chain of survival’ has been used to define the important links in the chain for the resuscitation process.10 The key links, which apply to both in- and out-of-hospital cardiac arrests, are: early recognition and the summoning of help, early basic life support (BLS), early access to defibrillation and early ALS, including postresuscitation care.10
RECENT CHANGES TO GUIDELINES
As a result of the science review published in 2005,12 a number of important changes have been made to the guidelines for both basic and ALS.
In summary, the BLS changes include:
These changes are discussed in more detail in the sections that follow.
BASIC LIFE SUPPORT
The general flow of BLS management is provided in the Australian Resuscitation Council BLS flowchart (www.resus.org.au; Figure 17.1).
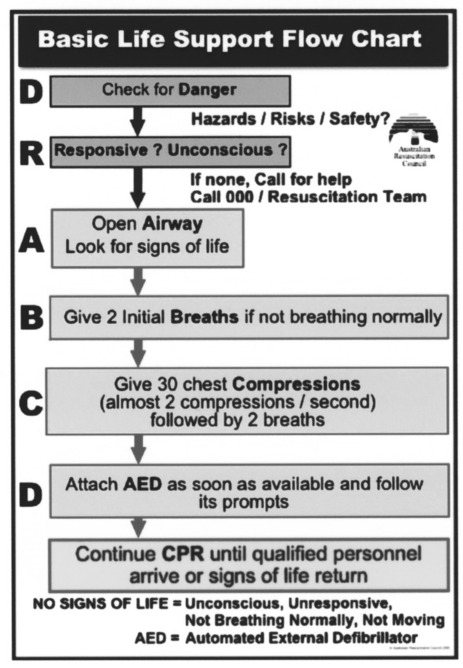
Figure 17.1 Basic life support flowchart.
(Reproduced from the Australian Resuscitation Council (www.resus.org.au), with permission.)
COMMENCEMENT OF CPR
The use of a pulse check as a means of determining the need for external cardiac compressions was downplayed in the 2000 guidelines, largely as a result of the review of a number of papers suggesting that even experienced providers may have difficulty in accurately assessing the presence or absence of a pulse.18 This was again confirmed in the current guidelines, where it has been recommended that CPR be commenced if the victim has no signs of life (unconscious/unresponsive, not breathing normally and not moving).16 An appropriately trained ALS provider can check for a central pulse (e.g. carotid) for up to 10 seconds during this period of assessment for signs of life.
EXTERNAL CARDIAC COMPRESSION
SITE OF COMPRESSION
The desired compression point for CPR in adults is over the lower half of the sternum. Compressions that are provided higher than this become less effective, and compressions lower than this are also less effective and have an increased risk of damage to intra-abdominal organs. Previous techniques that were widely taught to find this compression point may have introduced delays in commencing and recommencing chest compressions. To minimise pauses between ventilations and compressions, it is reasonable for laypeople and health care professionals to be taught to position the heel of their dominant hand in the centre of the chest of an adult victim (with the non-dominant hand on top).2
RATE OF COMPRESSION
The optimal rate of cardiac compression during cardiac arrest in adults has not yet been determined.2 In a recent human study,19 lower rates (e.g. < 80/min) were associated with worse outcomes and higher rates (> 120/min) with more fatigue and no benefits. It is recommended that chest compressions should be performed at a rate of approximately 100 compressions/minute.
DEPTH OF COMPRESSION
The ideal depth of compression is unknown. Compression depth is usually inadequate when it is measured in either manikin studies or actual cardiac arrests, and increasing depth of compression appears to be associated with higher defibrillation success.20 It is currently recommended that, when performing chest compressions in adults, the chest should be compressed by at least 4–5 cm (or approximately one-third of its depth).
MINIMISE INTERRUPTIONS TO COMPRESSIONS
Interruptions in chest compressions (‘hands-off time’) are common, often prolonged, and are associated with a decrease in coronary perfusion pressure and a deceased likelihood of defibrillation success.20–22 These adverse effects commence within 10 seconds, but appear to be at least partially reversible with the recommencement of chest compressions.23 It is recommended that CPR (initial breaths, then chest compressions) be commenced as soon as the victim is confirmed to have no signs of life. Pauses in compressions for rhythm recognition or specific interventions (such as ventilations, defibrillation or intubation) should be minimised.
COMPRESSION–VENTILATION RATIO
The minute ventilation requirements during cardiac arrest are less than that in the non-arrested state, so the respiratory rate can be decreased. To increase the number of compressions given per minute, minimise interruptions to chest compressions and simplify instruction for teaching and skills retention, a single compression-to-ventilation ratio of 30:2 is recommended for adult BLS before the airway is secured (irrespective of the number of rescuers).2 The tidal breath should be delivered within 1 second, and the desired tidal volume to be delivered is one that results in a visible chest rise.2
MONITORING THE QUALITY OF CPR
A number of different techniques are available to monitor the quality of CPR, some of which are more applicable toALS. Simple monitoring techniques include observation of the rate, depth and positioning of chest compressions, the rate and depth of ventilation and palpation of central pulses. Additional monitoring techniques that can be used include end-tidal carbon dioxide (Table 17.1), mechanical devices (e.g. for monitoring the depth of compressions) and new monitor/defibrillators (e.g. for monitoring the depth and rate of compressions and ventilation). Feedback from these devices can improve the quality of CPR and should result in improved outcomes.24
Table 17.1 Utility of end-tidal carbon dioxide (ETCO2) monitoring during cardiac arrest24
| Cardiovascular (absolute value of ETCO2) |
| Falls immediately at the onset of cardiac arrest |
| Increases immediately with chest compressions |
| Provides a linear correlation with cardiac index |
| Allows early detection of return of spontaneous circulation (sudden increase) |
| Respiratory (ETCO2 waveform) |
| Allows assessment of endotracheal tube placement |
| Allows assessment of expiratory flow limitation |
| Prognosis (absolute value of ETCO2) |
| Predicts successful resuscitation |
‘COMPRESSION-ONLY’ CPR
Increasing anxiety about the performance of mouth-to-mouth ventilation has required the consideration of an alternative approach to traditional bystander CPR. A number of animal studies have suggested that ventilation may not be necessary during the initial phase of resuscitation from an arrest of a cardiac cause (e.g. where VF was electrically induced).2 Recent research in human out-of-hospital cardiac arrests suggests that outcomes are not worse and may actually be better if ventilation is not initially attempted,25,26 although no studies have compared ‘compression-only’ CPR with the BLS protocols that are currently recommended. It is recommended that if rescuers are unable, not trained, or unwilling to perform mouth-to-mouth ventilation (rescue breathing) then they should perform ‘compression-only’ CPR.
DEFIBRILLATION
EARLY DEFIBRILLATION VERSUS CPR BEFORE DEFIBRILLATION
The timing of defibrillation with regard to other interventions appears crucial. The traditional approach to the treatment of a shockable rhythm during cardiac arrest has been to perform defibrillation as soon as possible. In the scenario of recent-onset VF, this still holds, and the best outcomes are associated with defibrillation within 3 minutes (e.g. in electrophysiology labs or coronary care units). However, in situations where the VF has persisted for more than a few minutes, an initial period of CPR may actually improve the likelihood of shock success, and result in better outcomes.23,27,28
WAVEFORM FOR DEFIBRILLATION
No specific defibrillator waveform (either monophasic or biphasic) is consistently associated with a greater incidence of return of spontaneous circulation (ROSC) or increased hospital discharge rates from cardiac arrest due to VF.29 Defibrillation with biphasic waveforms (either truncated exponential or rectilinear), using equal or lower energy levels, appears at least as effective for termination of VF as monophasic waveforms.30,31
ENERGY LEVELS
Recommendations for energy levels to be used for defibrillation vary according to the type of defibrillator (and the specific waveform) that the rescuers are using. Previous recommendations regarding energy levels were based on studies using monophasic waveforms that demonstrated increased heart block with higher energy levels. Current recommendations are based on maximising the likelihood of the success of each shock. The recommended energy level for defibrillation in adults where monophasic defibrillators are used is 360 J for all shocks. When using biphasic waveforms, the energy level should be set at 200 J for all shocks, unless there are relevant clinical data for the specific defibrillator that suggest that an alternative energy level provides adequate shock success (e.g. > 90%). There is no consistent evidence (e.g. survival benefit) to suggest that an escalation of energy levels is required for subsequent shocks.29,32
SINGLE-SHOCK TECHNIQUE
The use of a single-shock strategy for defibrillation is now recommended (i.e. deliver a single shock and then immediately commence CPR, rather than deliver up to three shocks in a sequence). This strategy has been proposed to decrease the interruptions to chest compressions which occur as a result of the repeated assessment of rhythm and signs of life that were inherent in the stacked-shock approach.29 This protocol would be of particular benefit in scenarios where there is a significant time required for rhythm recognition and recharging of the defibrillator (i.e. > 10 seconds), such as with AEDs. The benefits of this strategy are clearly dependent on the quality of CPR, as the next shock will be delayed for at least 2 minutes while CPR is performed.
The Australian Resuscitation Council does however recommend the retention of a stacked-shock strategy (up to three shocks as necessary) in a specific circumstance: for the first defibrillation attempt in a witnessed arrest, where a manual defibrillator is immediately available, and the time required for rhythm recognition and charging of the defibrillator is short (e.g. < 10 seconds), resulting in delivery of the (up to) three shocks within 30 seconds. All subsequent shocks should be given using a single-shock strategy (see www.resus.org.au).
ADVANCED LIFE SUPPORT
ADVANCED LIFE SUPPORT FLOWCHART
The recommended sequence of treatment to be followed is designated on the ALS flowchart of the Australian Resuscitation Council (www.resus.org.au; Figure 17.2). This is designed to be used as an aide-mémoire and a teaching tool.
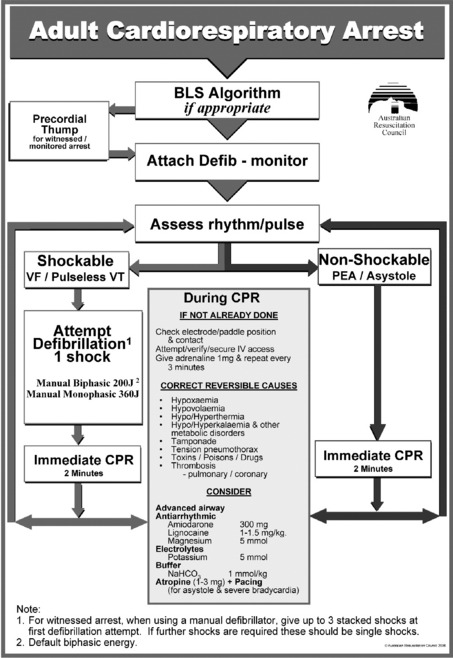
Figure 17.2 Advanced life support flowchart.
(Reproduced from the Australian Resuscitation Council (www.resus.org.au), with permission.)



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


