Fig. 8.1
A possible algorithm/pathway for diagnosis and treatment of arrhythmias in patients with channelopathies
Table 8.1
Conditions that can cause PVT/VF and potential therapies
Clues | Test to consider | Diagnoses | Therapies |
|---|---|---|---|
Long QT/T wave alternans TdP History of seizures Specific triggers (loud noise) | ECG/monitor Epinephrine challenge Exercise stress test Genetic testing | Congenital LQTS | Beta-blockers Avoid QT-prolonging drugs In LQT3: mexiletine/flecainide PM/ICD Stellatectomy |
Incomplete RBBB with STE in leads V1–V2 Fever | ECG Drug challenge Genetic testing | BrS | Isoproterenol/quinidine Antipyretic Ablation ICD |
J-point elevation | ECG | Early repolarization | ICD |
Short QT interval | ECG | SQTS | ICD Quinidine or sotalol |
Bidirectional VT exercise induced | Exercise stress test Genetic testing | CPVT Andersen-Tawil syndrome | Beta-blockers/flecainide/verapamil ICD |
8.5 Indications for Hospitalization, Follow-Up, and Referral
Following the arrhythmic index event, channelopathy patient should be reevaluated for risk stratification and prevention of recurrences. Expert centers with a focus on inherited arrhythmias should be involved in complex cases [4].
Atrial arrhythmias in low-risk patients could be managed in out-of-hospital setting with referral to arrhythmia experts to set up indication for pharmacological or non-pharmacological strategy. Thromboembolism should be managed according to AF guidelines using CHA2DS2VASC score [20]. First line therapy consists in avoiding potentially pro-arrhythmic drugs and conditions: a complete list should be supplied to the patient and to the general practitioner.
CPVT and LQT patients should be advised to limit/avoid competitive sport, strenuous exercise, and exposure to stressful environments (which in LQT2 should include exposure to loud/abrupt noises, i.e., alarm bell); Brugada patients should avoid excessive alcohol intake and large meals and should be advised to a prompt treatment of fever [45].
Syncope and life-threatening arrhythmias require hospitalization.
Aborted sudden death and sustained ventricular arrhythmias require an ICD for secondary prevention [4, 15, 31, 45] with or without adjunctive therapy.
CPVT and LQTS patients should be treated with beta-blockers: nadolol and propranolol are the drugs of choice [1, 4, 33]; in patients with recurrent symptoms/arrhythmias already on beta-blockers, it should be considered flecainide for CPVT patients [33] and flecainide or ranolazine or mexiletine in LQT3 patients [4]; ICD and left cardiac denervation should be considered in patients refractory to pharmacological therapy [4, 33]. Repeated exercise stress test is used in CPVT patients to evaluate drug efficacy.
Brugada and SQTS patients symptomatic for syncope should be treated with ICD; quinidine therapy could be used as adjunctive therapy or in cases in which ICD is refused or contraindicated or in recurrent appropriate ICD intervention [22, 26].
All clinically diagnosed patients with LQTS and CPVT should undergo genetic evaluation if not previously performed, and it can be useful in Brugada (type1) patients and SQTS [42]. Routine genetic testing is not indicated for the survivor of an unexplained out-of-hospital cardiac arrest in the absence of a clinical index of suspicion for a specific cardiomyopathy or channelopathy [42] (Figs. 8.2 and 8.3)
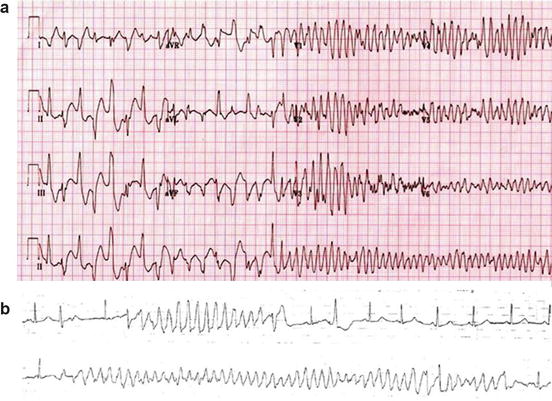
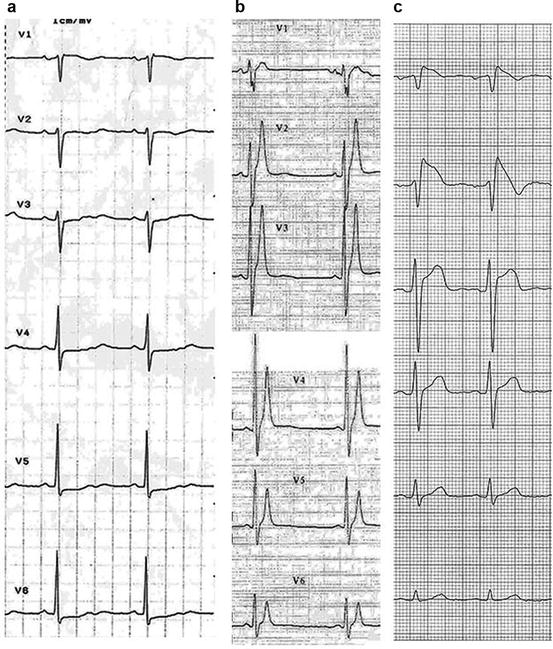
Fig. 8.2
Panel (a):12-lead ECG from a 9-year-old boy with ryanodine-positive CPVT shows a transition from triggered bidirectional ventricular tachycardia followed by brief polymorphic ventricular tachycardia to reentrant ventricular fibrillation. With permission from Elsevier Roses-Noguer F. et al. [43]: Copyright © 2014 Heart Rhythm Society. Panel (b): torsades de point. With permission from Van der Heide et al. [44]
Fig. 8.3
Precordial leads ECG in patients with panel (a), long QT syndrome, heart rate 58 beats per minute, QTc 600 ms; panel (b), short QT syndrome, heart rate 52 beats per minute (bpm), QT 280 ms*; panel (c), Brugada syndrome, coved ST elevation in V1–V2. *With permission from Gaita F. et al. [7]
References
1.
2.
Patel C, Burke JF, Patel H, et al. Is there a significant transmural gradient in repolarization time in the intact heart? Cellular basis of the T wave: a century of controversy. Circ Arrhythm Electrophysiol. 2009;2(1):80–8.PubMedPubMedCentralCrossRef
3.
4.
5.
Related posts:
 Management of Arrhythmic Patients in the Emergency Department: General Principles
Management of Arrhythmic Patients in the Emergency Department: General Principles
 Syncope: First Evaluation and Management in the Emergency Department
Acute Management of Patients with Arrhythmias and Non-cardiac Diseases: Metabolite Disorders and Ion Disturbances
Syncope: First Evaluation and Management in the Emergency Department
Acute Management of Patients with Arrhythmias and Non-cardiac Diseases: Metabolite Disorders and Ion Disturbances
 Cardiac Arrhythmias in Drug Abuse and Intoxication
Cardiac Arrhythmias in Drug Abuse and Intoxication
 Atrial Flutter and Fibrillation in the Emergency Setting
Atrial Flutter and Fibrillation in the Emergency Setting
 Wide QRS Complex Tachycardia in the Emergency Setting
Wide QRS Complex Tachycardia in the Emergency Setting
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


