Chapter 109 Accidental Hypothermia
Humans have a high capacity to dissipate heat and a relative poor capacity to increase heat production. As such, humans rely heavily on environmental regulation in the form of clothing and warm shelter to maintain normal body temperature. Thermoregulation is controlled by the hypothalamus. Heat production increases with movement. Shivering increases the rate of heat production three to five times above resting levels, but at the cost of greatly increased oxygen consumption. There are four primary means of heat loss: (1) conduction, (2) convection, (3) radiation, and (4) evaporation. Changes in the environment can radically increase heat loss (e.g., cold-water immersion can increase conductive heat loss by a factor of 32).1 Susceptibility to heat loss is greater in children than in adults because of a large surface area relative to body mass and less subcutaneous tissue, but severe accidental hypothermia is uncommonly encountered in most pediatric intensive care units. Neonates have a capacity for nonshivering thermogenesis, primarily by metabolism of brown fat; however, this is at the cost of greatly increased oxygen consumption. Neonates are therefore extremely sensitive to relatively minor deviations from neutral thermal environment.
There is no uniformity in the definition of hypothermia. The 2005 European Resuscitation Council Guidelines for Resuscitation classify a core temperature of 35° C to 32° C as mild hypothermia, 32° C to 30° C as moderate hypothermia, and less than 30° C as severe hypothermia.2 Hypothermia is further classified as accidental or intentional (as in cardiopulmonary bypass) and primary or secondary. Primary accidental hypothermia is due to environmental exposure, with no underlying medical condition causing disruption of temperature regulation.
Pathophysiology
The body can compensate to a great degree for mild hypothermia. The hypothalamus sends signals that produce cutaneous vasoconstriction, increased muscle tone, and metabolic rate. When muscle tone reaches a certain level, shivering thermogenesis begins. The clinical manifestations depend on the severity, acuity, and duration of temperature reduction; the patient’s age; premorbid conditions; and superimposed disease states. Each organ system may be affected by hypothermia.3,4
Central Nervous System
Central nervous system dysfunction is progressive. Cerebral oxygen consumption decreases in proportion to the reduction in metabolism. Cerebral blood flow decreases 6% to 7% for each 1° C decrease in temperature.1 Mild hypothermia may be associated with confusion, dysarthria, and impaired judgment.3–5 Deep tendon reflexes are depressed at core temperature lower than 32° C because of slowed peripheral nerve conduction. As body temperature drops, many patients no longer complain of cold. Shivering thermogenesis ceases at approximately 31° C. Pupillary responses decline and dilated unreactive pupils may be noted at temperatures lower than 30° C. Patients may experience hallucinations and sometimes paradoxically remove their clothes. The electroencephalogram (EEG) shows abnormal activity at temperatures less than 32° C, and at 20° C the EEG may appear consistent with brain death.1
Cardiovascular System
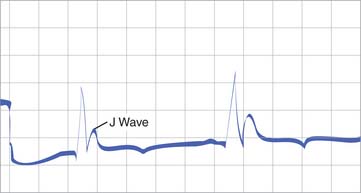
The initial cardiovascular responses are vasoconstriction, tachycardia, and increased cardiac output.5 Further hypothermia results in decreased pacemaker and conduction velocity, causing bradycardia, heart block, and prolongation of PR, QRS, and QT intervals. Bradycardia becomes severe by 32° C. The myocardium becomes irritable and arrhythmias are common when core temperature reaches 30° C. The electrocardiogram may show characteristic J or Osborne wave following the QRS complex (Figure 109-1).1,6–10 The presence of this wave is not pathognomonic for hypothermia and has no prognostic implications.11 Myocardial contractility, systemic blood pressure, and cardiac output are often decreased dramatically in patients who have severe hypothermia. These changes may be persistent during rewarming.12 Patients with hypothermia generally are volume contracted because of cold-induced diuresis.1,5,13
Respiratory System
Hypothermia affects tissue oxygenation through several complex physiologic mechanisms. Initially, the respiratory rate may be increased. As hypothermia worsens, the respiratory center becomes depressed and hypoventilation causes carbon dioxide retention, although the increase in carbon dioxide is blunted because of decreased production with increasing hypothermia. Respiratory arrest is a late occurrence. Suppression of cough and mucociliary reflexes leads to atelectasis and pneumonia.5 Oxygen delivery to the tissues is further compromised through the shifting of the oxyhemoglobin dissociation curve to the left.1 Blood gas analyzers warm blood to 37° C before analysis.14 In patients with hypothermia, arterial blood gases show higher oxygen and carbon dioxide levels and a lower pH than a patient’s actual values. The best approach to interpretation is to compare the uncorrected blood gas values with the normal values at 37° C (alpha-stat strategy).15–17
Renal System
Renal injury may occur either because of hypothermia or during the rewarming process.18 The mechanisms involved in cold diuresis may include peripheral vasoconstriction and blunted response to antidiuretic hormone. Renal vasoconstriction and ischemia to the kidney may lead to oliguria and acute tubular necrosis in those with severe hypothermia.5 Progressive hypokalemia develops during hypothermia, probably because of the shifting of potassium from extracellular to intracellular compartment, and significant hyperkalemia may develop during rewarming.19–21 Metabolic and respiratory acidoses are not uncommon findings in patients who have moderate and severe hypothermia.14 Hemodialysis has been required for renal failure and may also be of use as an active rewarming strategy.22
Coagulation
Hypothermia inhibits the intrinsic and extrinsic pathways in the clotting process. The degree of coagulopathy, however, is often underestimated because dynamic coagulation tests are generally performed at 37° C in the laboratory. Thrombocytopenia, from bone marrow suppression and splenic sequestration, and platelet dysfunction are common.1,15
Treatment
The key to rescue in all individuals with hypothermia is prevention of further heat loss, careful transport, and rewarming.1 Wet clothes should be removed, and the individuals should be insulated and shielded from wind and cold. Paying special attention to the head and neck is important because radiant heat loss from those areas can be profound. Detecting signs of life in patients with deep hypothermia may be difficult, and the rescuer should therefore assess breathing and then pulse for 30 to 60 seconds to confirm respiratory arrest, cardiac arrest, or bradycardia. Chest compressions should be started immediately if the patient is pulseless with no detectable signs of circulation. Endotracheal intubation should be performed if the patient with hypothermia is unconscious or if ventilation is inadequate. Anecdotal reports of sudden cardiac death associated with tracheal intubation appear to be exaggerated, particularly if the patient is adequately preoxygenated and the procedure is performed in a gentle manner. If cervical spine injury is suspected, the neutral position must be maintained with manual cervical stabilization. Care should be taken not to overventilate the patient’s lungs because this can increase ventricular irritability.23 Rewarming by the administration of warmed humidified oxygen (42° C to 46° C) and warmed saline (43° C) should begin as soon as possible. Ringer’s lactate solution is not recommended because a hypothermic liver cannot metabolize lactate. Defibrillation can be tried up to three times for ventricular tachycardia or fibrillation. If arrhythmia is resistant to three shocks in a patient with deep hypothermia, then further defibrillation attempts should be deferred until core temperature is increased. The hypothermic heart may also have a reduced response to cardioactive drugs and pacemaker stimulation.1,2 Therefore the efficacy of drugs in severe hypothermia is limited and there is concern that medications can accumulate to toxic levels if they are administered repeatedly.24–26
No randomized controlled clinical trials in which rewarming methods are compared exist.16 The rewarming of patients who are conscious and who have only mild or moderate hypothermia can be achieved with passive techniques (e.g., blankets, warm shelter). Management of severe hypothermia in the field is more controversial. Active external rewarming with heat devices (e.g., forced air, radiant heat, warm bath, warm packs) requires careful monitoring and should therefore be used with caution. The concerns are core temperature afterdrop and rewarming shock.1,4,15,16,27–29 The term core temperature afterdrop refers to a continued decrease in core temperature and associated clinical deterioration of a patient after rewarming has begun. Some researchers suggest that peripheral vasodilatation due to external rewarming leads to circulation of cold blood into the core of the body.28 Simple equilibration of temperature between the periphery and the core is probably a far more important mechanism. Heat flows from the core to the periphery during cooling and the opposite is true during external rewarming. However, there is a delay in the reversal of temperature flow in deeper tissues and the core temperature may decrease for some time after rewarming has begun. It follows that the magnitude of core temperature afterdrop is greater if cooling is rapid because the temperature gradient between the surface and core is greater.30 The hazard of afterdrop may be overrated. It is not uncommon, though, for patients with hypothermia to have “rewarming shock” or “postrescue collapse.”1,29,31,33 However, the underlying pathophysiologic condition behind this remains obscure and several mechanisms may contribute including myocardial dysfunction, decreased vascular tone, derangements of the microcirculation, and hypoxia or sudden changes in pH.12,29,31 Depleted intravascular volume may also contribute to the development of shock, and most patients will benefit from volume expansion.1,14 The patient should be kept horizontal to minimize hypotension and sympathetic discharge. Avoiding excessive activity and abrupt movements of patients with hypothermia is important because this may precipitate cardiac dysrhythmias.
Techniques that can be used for in-hospital rewarming of hemodynamically stable patients include continued active external rewarming, and active core rewarming with lavage of body cavities or warming of blood with extracorporal circulation. Active external rewarming can be effective, and there are several reports of successful use of active external rewarming or minimally invasive techniques in children with severe hypothermia and cardiac arrest.33–41 Cardiopulmonary bypass should be considered in patients, even those without cardiac arrest, who suffer from severe hypothermia. It remains the preferred method to resuscitate patients with severe hypothermia and cardiac arrest or cardiovascular instability.1,2,42–52 In most reports, partial bypass from femoral artery to femoral vein is described in adult patients. Full bypass with a median sternotomy may be preferable in small children.44,53 Other methods of core rewarming that can be considered include peritoneal lavage with heated potassium-free dialysate, thoracic lavage, and the use of esophageal rewarming tubes.54–57








