Blood ethanol concentration as indicated in the breath (top); serum sodium (middle); and the fluid absorption rate as obtained by careful measurements of the volumetric fluid balance corrected from blood loss over 5- or 10-min periods (bottom) in one patient undergoing transurethral resection of the prostate. The route of fluid uptake is intravascular.
One important issue is that the anesthetist must be aware of how the alcolmeter is calibrated (for blood or breath) to consult the correct nomogram when obtaining an estimate of how much fluid that has been absorbed. A challenge is that intravascular and extravascular absorption give rise to different patterns and levels of breath ethanol concentrations. The extravascular type gives a slowly rising ethanol concentration that remains high when irrigation has stopped (Figure 33.2). With the more common intravascular type of fluid absorption, elevations of the breath ethanol concentration can occur much faster and a drop is seen within a few minutes after the irrigation has stopped.
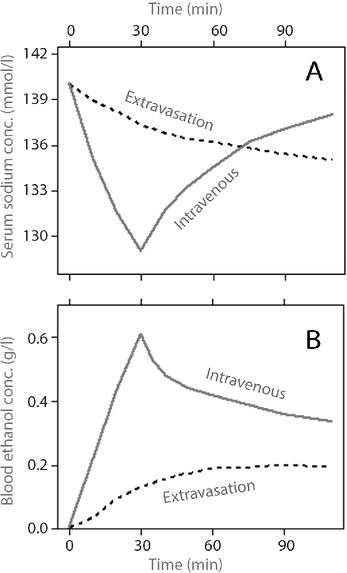
Expected course of serum sodium (A) and blood ethanol concentration (B) (the latter measured in the expired breath) during and after TURP during which absorption of 2 liters of irrigating fluid containing glycine 1.5% and ethanol 1% has occurred over 30 min, depending on the route of absorption.
Measuring serum sodium has the purpose of confirming that fluid absorption is the cause of the symptoms. On the other hand, non-invasive methods that can be repeated perioperatively, such as volumetric balance and the ethanol method, open up the possibility of preventing large-scale fluid absorption from occurring. Once data indicate that 1 liter of fluid has been absorbed it is suggested that the operation should be concluded earlier than planned, and after 2 liters it becomes even more important to stop surgery. An early indication that irrigating fluid has been absorbed allows the optimal level of postoperative care to be chosen and also the initiation of the earliest possible treatment.
Nomograms for how to estimate fluid absorption are shown in Figures 33.3 and 33.4. Regression equations have also been developed for calculation of fluid absorption in the scientific setting (see Box 33.1).
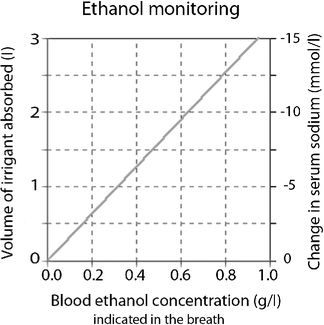
Nomogram for quick reference between the volume of irrigant absorbed and the breath ethanol concentration (calibrated to blood ethanol) and, if the fluid is electrolyte-free, the corresponding decrease in serum sodium. The volume of irrigant absorbed is given from the average absorption time during TURP, which is 20 min. The median absolute residual error is 146 ml and R2 for the regression is 0.80.
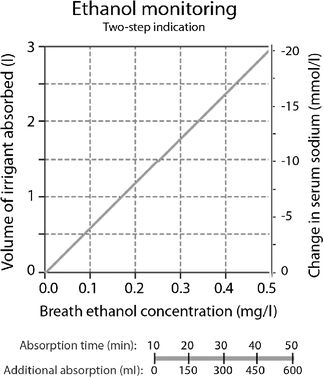
Nomogram for estimating the volume of irrigant absorbed from the breath ethanol concentration (not calibrated to blood ethanol) at any time during TURP. If the fluid is electrolyte-free, the corresponding decrease in serum sodium is also predicted. To estimate intravascular fluid absorption, first use the upper nomogram and add the effect of distribution and elimination by using the scale below. The median absolute residual error is 118 ml and R2 for the regression 0.90.The accompanying decrease in serum sodium inflicted by the use of electrolyte-free irrigating fluid is obtained directly from the upper nomogram.
An equation recommended for scientific reports is one that is based on 10-min measurements throughout 90 TURPs [49]. Here, the equation gives the absorbed volume in 10-min increments that must be summed to give the total absorption:

where ethanoli is the blood ethanol concentration as indicated in the breath at the beginning of the 10-min period, and ∆ethanol is the change in concentration during that 10-min period.
Assume that we have a TURP operation in which one ethanol measurement is made at the end of three successive 10-min periods. The readings are 0.15, 0.25, and 0.30 g/l. When the reading is zero, the equation should not be applied. Inserting the data series given above, this equation provides the following output for the three 10-min periods mentioned above:
Absorption = (2,140 + 3,430 × 0) × 0.15 + (44 + 806 × 0) = 321 + 44 = 365 ml
Absorption = (2,140 + 3,430 × 0.15) × 0.10 + (44 + 806 × 0.15) = 265 + 165 = 430 ml
Absorption = (2,140 + 3,430 × 0.25) × 0.05 + (44 + 806 × 0.25) = 150 + 246 = 396 ml
The total absorption during the 30-min surgical procedure is the sum of these three 10-min calculations, i.e. 365, (365 + 430) = 795, and finally (365 + 430 + 396) = 1,191 ml. The median absolute residual error is approximately 100 ml, and the equation can also be applied for decreasing concentrations, as some ongoing absorption is needed to maintain an already elevated ethanol level. Decreasing ethanol concentrations can be handled by letting ∆ethanol attain negative values. Continued absorption is needed to maintain a raised ethanol level, and more is required to maintain a high concentration than a low because most of the decrease is due to distribution. Arrested absorption typically results in a rapid fall in the ethanol level provided that absorption has occurred by the intravascular route.
From [48], reproduced courtesy of Acta Anaesthesiologica Scandinavica.
Prevention
Fluid absorption and blood loss is reduced, but not eliminated, by vaporizing rather than resecting tissue.
The irrigating fluid used during TURP might be evacuated through a suprapubic trocar. This allows the use of continuous irrigation at a low fluid pressure, which speeds up the operation but increases the use of irrigating fluid. Low-pressure irrigation limits or prevents fluid absorption as long as the outflow is not obstructed by debris and blood clots.
Fluid absorption varies between surgeons and depends on their skill in avoiding prostatic capsule perforations or the opening up of venous sinuses.
There is a belief among urologists that dangerous fluid absorption during TURP can be prevented by limiting the operating time to 1 hour. However, the odds for absorption involve a similar likelihood over time, which accumulates to a gradually increased total risk.[2]. Hence, massive fluid absorption might already be at hand after 20 min of surgery.
Placing the irrigating fluid bag at low height above the operating table is of little help because urologists tend to operate at a much lower fluid pressure than made possible by the bag height.[40,41]
The bipolar resection technique allows the use of normal saline for irrigation, and is often claimed to prevent the TUR syndrome. Experience with fluid overload during bipolar resection is still limited. There is no reason to believe that fluid absorption will be less frequent, but the TUR syndrome is likely to have a different appearance.
Treatment
The TUR syndrome requires general supportive measures if breathing and/or consciousness are affected. Severe hypotension should be treated promptly with colloid volume loading, intravenous calcium, and adrenergic drugs.
Hypertonic saline should be infused when the hemodynamics is under control. The indication requires either that symptoms have developed or that the serum sodium concentration has fallen to below 120 mmol/l, which corresponds to absorption of approximately 3.5 liters of fluid. Hypertonic saline combats cerebral edema and expands the plasma volume, reduces cellular swelling, and increases urinary excretion.
Both experimental [42] and clinical [43,44] studies support the usefulness of treating the TUR syndrome with hypertonic saline. Above all, raising the serum sodium level is most essential in menstruating women because they are more prone to develop brain damage from hyponatremia than other patients.
Rapid correction of chronic hyponatremia might induce pontine myelinolysis but this is not the experience with acute hyponatremia. An infusion of 250 ml of 7.5% NaCl can be started slowly and another bag added later if necessary. Raising the serum sodium level by 1 mmol/l per hour has been suggested as a safe rate,[44] but hypertonic saline has not been reported to induce pontine myelinolysis when given faster. Treatment should stop when serum sodium has reached 130 mmol/l as there is a risk of over-correction.
Diuretic treatment is imperative in case pulmonary edema or renal failure develops. However, such drugs aggravate hypotension and hyponatremia and should therefore be withheld until the hemodynamic situation is under control and a drip of hypertonic saline is ongoing. The value of diuretics has not been evaluated in randomized clinical studies, but without diuretics absorbed electrolyte-free irrigating fluid in excess of 1 liter is strongly associated with a positive fluid balance 24 hours after TURP.[45] Hypertonic mannitol might be superior to furosemide if used early on after the surgery.[46]
Massive extravasation to the periprostatic or intraperitoneal spaces can be treated with surgical drainage. Here, electrolytes from the ECF enter the pool of irrigating fluid more quickly than the pool is absorbed by the circulation.[47] Hence, surgical drainage removes electrolytes from the body and they need to be replaced. Special attention should be given to the high risk of arterial hypotension and associated oliguria.[15]
Large-scale fluid absorption with normal saline is a possibility during bipolar resection. Treatment should probably be limited to general supportive measures and diuretics. Hypertonic saline is not indicated.
References
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


