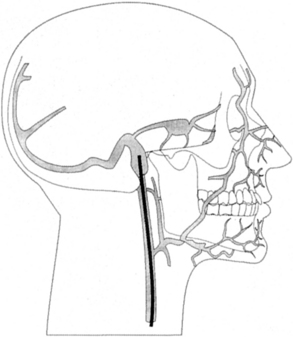
PROCEDURE 90 Jugular venous oxygen saturation (SjVO2) catheters detect the oxygen saturation of hemoglobin in the blood after cerebral perfusion. The direct and derived parameters obtained from jugular venous oxygen saturation catheters reflect global cerebral oxygenation. Inclusion of jugular venous oxygen saturation data in the clinical management of the patient may prevent the secondary brain injury that occurs as a result of an imbalance between cerebral oxygen delivery and cerebral oxygen demand.2,43 • Fundamental understanding of neuroanatomy and physiology is needed. • Knowledge of aseptic and sterile technique is necessary. • The secondary brain injury that occurs as a result of an imbalance in oxygen supply and demand is accompanied by increased intracranial pressure (ICP), potential or actual compromise in cerebral perfusion, or other alterations that lead to cerebral ischemia.4,29,32 • Cerebral ischemia results in poor outcomes in critically ill patients.2,3,5,8,19,35,36 • Normal jugular venous oxygen saturation (SjVO2) values range from 55% to 70%.7,13,33,35,38,40 SjVO2 values less than 45% to 50% indicate relative cerebral ischemia, especially with frequent desaturations.7,9,10,12,13,18,25,39 • SjVO2 values greater than 70% may demonstrate hyperemia.8,21,23,26,28,31,32,40 Hyperemia occurs as the result of an increase in cerebral blood flow or hyperdilation of distal cerebrovascular resistance beds and is frequently accompanied by increases in ICP.20 • SjVO2 monitoring is recommended in patients at risk for global cerebral hypoxia, including those with acute severe traumatic brain injury (Glasgow Coma Scale [GCS] score equal to or less than 8)6,19,26,36,38; aneurysmal subarachnoid hemorrhage, including vasospasm9,24; intraoperative monitoring during craniotomy for tumor, abscess, aneurysm, arteriovenous malformation, spontaneous intracerebral hemorrhage,24 and carotid endarterectomy for carotid stenosis; intraoperative monitoring during cardiac surgery, especially hypothermic cardiopulmonary bypass and rewarming; patients successfully resuscitated; ICP and cerebral perfusion pressure (CPP) management; controlled hyperventilation for increased ICP; and barbiturate coma for refractory increased ICP.4 • Contraindications for SjVO2 monitoring include coagulopathies, cervical spine injury, local neck trauma, and impaired cerebral venous drainage.4 • The SjVO2 catheter is placed retrograde in the dominant internal jugular vein (usually the right internal jugular vein).11,14–17,23,33 • The SjVO2 catheter tip is positioned at the location of the jugular bulb of the internal jugular vein.20,23 This is at the mastoid process, approximately at the C1-C2 interspace (Fig. 90-1).1 Ultrasound scan devices may be used to locate the jugular bulb to ease bedside placement. Figure 90-1 Placement of the jugular bulb venous catheter. (From Kidd KC, Criddle L: Using jugular venous catheters in patients with traumatic brain injury, Crit Care Nurse 21:16-22, 2001.) • A decrease in SjVO2 (55%) may be due to increased demand as a result of pain, hyperthermia, shivering, agitation, or seizures. It may also be due to decreased delivery as a result of hyperventilation (hypocarbia), decreased cardiac output, hypotension, hypovolemia, anemia, hypoxia, and sepsis.4 • An increase in SjVO2 (70%) may be due to decreased demand as the result of hypothermia, anesthesia, paralytics, and sepsis. It may also be due to increased delivery.4 • Derived SjVO2 parameters include arteriovenous jugular oxygen content difference (AvjDO2), the cerebral extraction of oxygen (CEO2), and the cerebral metabolic rate of oxygen consumption (CMRO2). • The technology used for continuous SjVO2 monitoring is oximetry, which is based on the unique light absorption spectrum of oxyhemoglobin.40 Oximetry requires calibration, either in vivo, within the patient’s jugular vein, or in vitro, calibration before insertion, outside the body. Formulas and normal ranges for SjVO2 catheter data and calculations are included in Tables 90-1 and 90-2. Clinical interventions based on SjVO2 data are shown in Table 90-3. Table 90-1 Formulas for Calculations Using SjVO2 Data Table 90-2 Normal Ranges for SjVO2 Data and Calculations
Jugular Venous Oxygen Saturation Monitoring: Insertion (Assist), Patient Care, Troubleshooting, and Removal
PREREQUISITE NURSING KNOWLEDGE
 AvjDO2 reflects the relationship between cerebral blood flow (CBF) and CMRO2.27,28,35,41,42
AvjDO2 reflects the relationship between cerebral blood flow (CBF) and CMRO2.27,28,35,41,42
 Normal range: 4.0 to 8.0 mL/dL
Normal range: 4.0 to 8.0 mL/dL
 Calculation requires data obtained from both systemic arterial and jugular venous blood gas analysis
Calculation requires data obtained from both systemic arterial and jugular venous blood gas analysis
 CEO2 reflects the influence of cerebral blood volume change (CBV) and its effect on CBF and CMRO2. Blood volume flow is not equal to blood volume.27,35,41,45
CEO2 reflects the influence of cerebral blood volume change (CBV) and its effect on CBF and CMRO2. Blood volume flow is not equal to blood volume.27,35,41,45
 CMRO2 is the energy needed for cellular function.35,41 This parameter includes knowledge of the cerebral blood flow and AvjDO2 and is less frequently calculated in the clinical setting. Normal CMRO2 is 3.2 mL/100 g/min.
CMRO2 is the energy needed for cellular function.35,41 This parameter includes knowledge of the cerebral blood flow and AvjDO2 and is less frequently calculated in the clinical setting. Normal CMRO2 is 3.2 mL/100 g/min.
Calculations
Formula
AvjDO2 (mL/dL)
CaO2 (mL/dL) − CjVO2 (mL/dL)
CEO2 (%)
SaO2 (%) − SjVO2 (%)





