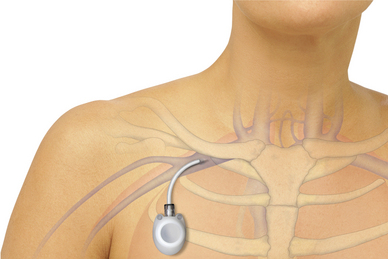
PROCEDURE 83 • Understanding of the implantable venous access device, including the septum and outer borders, is needed. • Knowledge of the anatomy of the venous system is necessary. • Understanding is needed of the principles of medication delivery. Intermittent use necessitates flushing with normal saline solution (NS) after each use and instillation of heparin as prescribed. • Understanding of the principles of aseptic and sterile technique is necessary. • The properties of chemotherapeutic or cytotoxic agents and preferred delivery techniques should be understood. • Understanding of the consequences of infiltration of vesicant substances is needed. • Implanted venous access devices are surgically placed, totally implanted in a cutaneous pocket (usually in the chest wall), and designed to provide venous access for intermittent or continuous infusions, maintaining a patient’s intact body image when not accessed. • Implanted devices consist of a slim tube or catheter connected to a reservoir, which is covered by a disc 2 to 3 cm in width (Figs. 83-1 and 83-2). The disc is made of silicone and is referred to as the septum. Provided a noncoring needle is used to access the septum, the septum is capable of resealing when deaccessed. The internal catheter is connected to the patient’s venous system and may consist of either silicone or polyurethane.5,15 • The implanted venous access device is percutaneously accessed with a noncoring needle. • The use of a noncoring needle allows for repeated access of the venous device without damage to the silicone core. • The noncoring needle chosen should be of optimal length, with the most common length for adults 1½ or 1¾ inches. Patients with increased subcutaneous tissue may need a longer needle for access. Too short a needle may cause the flanges to press against the skin surrounding the portal chamber, leading to patient discomfort and possibly resulting in damage to the skin overlying the venous access device. Too long a needle may result in a rocking motion that can cause discomfort, possible migration out of the portal septum, or damage to the integrity of the septum, impairing it for further use. • Skin antiseptic solution (e.g., 2% chlorhexidine–based solution) • Prepierced needleless injection cap • Heparin flush, 100 units/mL concentration • Central venous catheter dressing change kit Additional equipment as needed includes the following:
![]() Implantable Venous Access Device: Access, Deaccess, and Care
Implantable Venous Access Device: Access, Deaccess, and Care
PREREQUISITE NURSING KNOWLEDGE
EQUIPMENT
PATIENT AND FAMILY EDUCATION
Related posts:
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 74: Pulmonary Artery Catheter Removal
74: Pulmonary Artery Catheter Removal
![]() 14: Tracheostomy Tube Care
14: Tracheostomy Tube Care
![]() 82: Central Venous Catheter Insertion (Assist)
82: Central Venous Catheter Insertion (Assist)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Anesthesia Key
Fastest Anesthesia & Intensive Care & Emergency Medicine Insight Engine