PROCEDURE 80 • An arterial blood gas (ABG) analysis measures the pH and the partial pressure of oxygen (PaO2) and carbon dioxide (PaCO2). ABG samples are also analyzed for oxygen saturation (SaO2) and for bicarbonate (HCO−3) values. These analyses are done primarily to evaluate a patient’s oxygenation status, acid-base balance, and ventilation.3,5 Additional laboratory tests (e.g., ammonia and lactate levels) can be performed on arterial blood samples. • Patient indications for ABGs vary and include patients with chronic obstructive pulmonary disease (COPD), acute respiratory distress syndrome (ARDS), and pneumonia. ABG analysis frequently is performed on patients in shock, receiving cardiopulmonary resuscitation (CPR), or experiencing changes in respiratory therapy or status.3,5 • Knowledge of principles of aseptic technique is necessary. • Knowledge is needed of the anatomy and physiology of the vasculature and adjacent structures. • The brachial artery is a continuation of the axillary artery in the upper extremity. It bifurcates just below the elbow (Fig. 80-1). From the bifurcation, the ulnar artery moves down the forearm on the medial side and the radial artery on the lateral side.20 • The preferred artery for arterial puncture is the radial artery. Although this artery is smaller than the ulnar artery, it is more superficial and can be more easily stabilized during the procedure.6 The use of the brachial artery is a safe and reliable alternative site for arterial puncture.16 • At times, the femoral artery is used for arterial puncture. The use of this artery can be technically difficult because of the proximity of the artery to the femoral vein (Fig. 80-2). • Arterial cannulation is considered for patients who need frequent arterial blood samples, continuous arterial pressure monitoring, or evaluation of vasoactive medication therapy (see Procedures 61 and 62).5 • The most common complications associated with arterial puncture include pain, vasospasm, hematoma formation, infection, hemorrhage, and neurovascular compromise.5,9,16,19 • Site selection proceeds as follows: • One prepackaged ABG kit that contains the following: • Appropriate laboratory form, specimen label • One pair of nonsterile examination gloves and eye protection • 1% lidocaine (without epinephrine), 1-mL, or eutectic mixture of local anesthetics (EMLA) cream Additional supplies as needed include the following:
![]() Arterial Puncture
Arterial Puncture
PREREQUISITE NURSING KNOWLEDGE
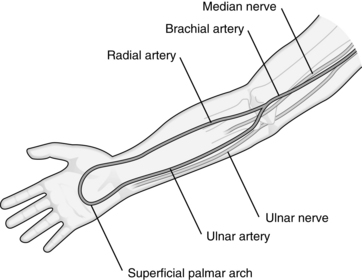
 Use the radial artery as first choice. The radial artery is small and easily stabilized as it passes over a bony groove located at the wrist (see Fig. 80-1).
Use the radial artery as first choice. The radial artery is small and easily stabilized as it passes over a bony groove located at the wrist (see Fig. 80-1).
 Use the brachial artery as second choice, except in the presence of poor pulsation from shock, obesity, or sclerotic vessel (e.g., because of previous cardiac catheterization). The brachial artery is larger than the radial artery. Hemostasis after arterial puncture is enhanced by its proximity to bone if the entry point is approximately 1.5 inches above the antecubital fossa (see Fig. 80-1).
Use the brachial artery as second choice, except in the presence of poor pulsation from shock, obesity, or sclerotic vessel (e.g., because of previous cardiac catheterization). The brachial artery is larger than the radial artery. Hemostasis after arterial puncture is enhanced by its proximity to bone if the entry point is approximately 1.5 inches above the antecubital fossa (see Fig. 80-1).
 Use the femoral artery in the case of cardiopulmonary arrest or altered perfusion to the upper extremities. The femoral artery is a large superficial artery located in the groin (see Fig. 80-2). It is easily palpated and punctured. Complications related to femoral artery puncture include hemorrhage and hematoma because bleeding can be difficult to control; inadvertent puncture of the femoral vein because of the close proximity of the vein to the artery; infection because aseptic technique in the groin area is difficult to maintain; and limb ischemia if the femoral artery is damaged.
Use the femoral artery in the case of cardiopulmonary arrest or altered perfusion to the upper extremities. The femoral artery is a large superficial artery located in the groin (see Fig. 80-2). It is easily palpated and punctured. Complications related to femoral artery puncture include hemorrhage and hematoma because bleeding can be difficult to control; inadvertent puncture of the femoral vein because of the close proximity of the vein to the artery; infection because aseptic technique in the groin area is difficult to maintain; and limb ischemia if the femoral artery is damaged.
EQUIPMENT
 One 20-gauge to 25-gauge, 1-inch to 1.5-inch hypodermic needle (note: longer needles are needed for brachial and femoral artery puncture)
One 20-gauge to 25-gauge, 1-inch to 1.5-inch hypodermic needle (note: longer needles are needed for brachial and femoral artery puncture)
 One 1- to 5-mL preheparinized (if available) syringe with a rubber stopper or cap
One 1- to 5-mL preheparinized (if available) syringe with a rubber stopper or cap
 One 1-mL ampule of sodium heparin, 1:1000 concentration (if preheparinized syringe is not available)
One 1-mL ampule of sodium heparin, 1:1000 concentration (if preheparinized syringe is not available)
 2% chlorhexidine–based antiseptic solution
2% chlorhexidine–based antiseptic solution
 One plastic bag (for transport of sample to laboratory)
One plastic bag (for transport of sample to laboratory)
PATIENT AND FAMILY EDUCATION
Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Anesthesia Key
Fastest Anesthesia & Intensive Care & Emergency Medicine Insight Engine