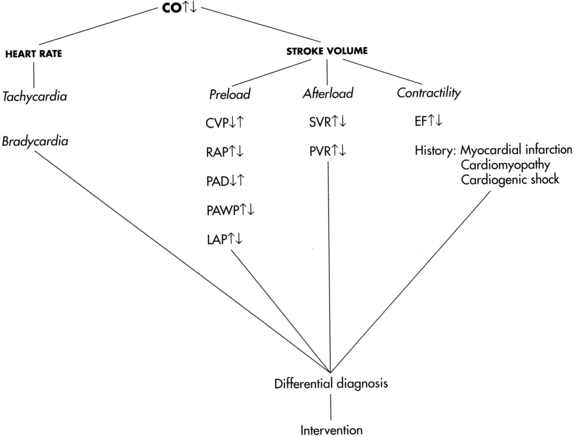
PROCEDURE 67 • Understanding of normal anatomy and physiology of the cardiovascular system and pulmonary system is necessary. • Understanding of basic dysrhythmia recognition and treatment of life-threatening dysrhythmias is needed. • Pathophysiologic changes associated with structural heart disease (e.g., ventricular dysfunction from myocardial infarction, diastolic or systolic changes and valve dysfunction) should be understood. • Understanding of the principles of aseptic technique is necessary. • Understanding of the pulmonary artery (PA) catheter (see Fig. 73-1), lumens and ports, and the location of the PA catheter in the heart and PA (see Fig. 73-2) is needed. • Multiple pressure transducer systems (see Procedure 76) should be understood. • Competence in the use and clinical application of hemodynamic waveforms and values obtained with a PA catheter is necessary. Hemodynamic waveform interpretation of right atrial pressure (RAP) or central venous pressure (CVP), pulmonary artery pressure (PAP), and pulmonary artery occlusion pressure (PAOP) or pulmonary artery wedge pressure (PAWP) provides confirmation of proper catheter placement. • Knowledge of vasoactive and inotropic medications and their effects on cardiac function, ventricular function, coronary vessels, and vascular smooth muscles is needed. • Cardiac output (CO) is defined as the amount of blood ejected by the left ventricle per minute and is the product of stroke volume (SV) and heart rate (HR). It is measured in liters per minute. • Normal CO is 4 to 8 L/min. The four physiologic factors that affect CO are preload, afterload, contractility, and heart rate. • Stroke volume is the amount of blood volume ejected from either ventricle during one beat. Left ventricular stroke volume is the difference between left ventricular end-diastolic volume and left ventricular end-systolic volume. Left ventricular stroke volume is normally 60 to 100 mL/beat. Major factors that influence stroke volume are preload, afterload, and contractility. • Right heart preload refers to the amount of blood in the right ventricle (RV) at the end of diastole and is measured by the RAP or CVP. Elevations in left heart filling pressures may be accompanied by parallel changes in RAP, especially in patients with left systolic ventricular dysfunction. Other factors that affect RAP are venous return, intravascular volume, vascular capacity, and pulmonary pressure. Right heart preload is increased in right heart failure, right ventricular infarction, pericardial tamponade, tension pneumothorax, tricuspid regurgitation, and fluid overload. Right heart preload is decreased in hypovolemic states. • Left heart preload refers to the amount of blood in the left ventricle (LV) at the end of diastole and is measured by the PAOP or PAWP. When LV preload or end-diastolic volume increases, the muscle fibers are stretched. The increased tension or force of contraction that accompanies an increase in diastolic filling is called the Frank-Starling law. The Frank-Starling law allows the heart to adjust its pumping ability to accommodate various levels of venous return. Note: In patients with advanced chronic LV dysfunction and remodeled hearts (spherical or globular-shaped LV instead of the normal elliptical-shaped LV), the Frank-Starling law does not apply. In these patients, muscle fibers of the heart are already maximally lengthened; as a result, the heart cannot respond significantly to increased filling or stretch with increased force of contraction. • Afterload refers to the force the ventricular myocardial fibers must overcome to shorten or contract. It is the force that resists contraction. The amount of force the LV must overcome influences the amount of blood ejected into the systemic circulation. Afterload is influenced by peripheral vascular resistance (the force opposing blood flow within the vessels), systolic blood pressure, systolic stress, and systolic impedance. Peripheral resistance is affected by the length and radius of the blood vessel, arterial blood pressure, and venous constriction or dilation. The systolic force of the heart is increased in conditions that cause vasoconstriction (increased afterload), including aortic stenosis, hypertension, or hyperviscosity of blood (e.g., polycythemia). The systolic force of the heart is decreased in conditions that cause vasodilation or decrease the viscosity of blood (e.g., anemia). Right ventricular afterload is measured as pulmonary vascular resistance. Left ventricular afterload is measured as systemic vascular resistance. • Contractility is defined as the ability of the myocardium to contract and eject blood into the pulmonary or systemic vasculature. Contractility is increased by sympathetic neural stimulation, the release of calcium, and norepinephrine and decreased by parasympathetic neural stimulation, acidosis, and hyperkalemia. Contractility and HR can be influenced by neural, humoral, and pharmacologic factors. • In addition to stroke volume, CO is affected by heart rate. Normally, nerves of the parasympathetic and sympathetic nervous system regulate heart rate through specialized cardiac electrical cells. Heart rate and rhythm are influenced by neural, humoral, and pharmacologic factors. Decreased HR can be the result of increased parasympathetic neural stimulation, decreased sympathetic neural stimulation, or decreased body temperature. Increased HR can be triggered by exercise, catecholamine release, or hypotension. At HRs greater than 180 beats/min, there may be inadequate time for diastolic filling, resulting in decreased CO. Because multiple factors regulate cardiac performance and impact CO, these factors must be assessed (Fig. 67-1). • Cardiac index adjusts the CO to an individual’s body size (square meter of body surface area). It is a more precise measurement of cardiac performance than CO. • Refer to Table 67-1 for normal hemodynamic values and calculations. Table 67-1 Adapted from Tuggle D: Optimizing hemodynamics: strategies for fluid and medication titration in shock. In Carlson K, editor: AACN advanced critical care nursing, St Louis, 2009, Saunders, 1106; and Ahrens T: Hemodynamic monitoring, Crit Care Nurs Clin N Am 11:19-31, 1999. • At the bedside, cardiac output measurements are obtained through a PA catheter via the intermittent bolus thermodilution CO method (TDCO) or the continuous CO (CCO) method. • The TDCO method proceeds as follows: • CO can be calculated from PA catheters with two types of thermistors: • The change in temperature over time is plotted as a curve and displayed on the bedside monitor screen. CO is mathematically calculated from the area under the curve and is displayed digitally and graphically on the monitor screen (Fig. 67-2). The area under the curve is inversely proportional to the rate of blood flow. Thus, a high CO is associated with a small area under the curve, whereas a low CO is associated with a large area under the curve (Fig. 67-3, A).
Cardiac Output Measurement Techniques (Invasive)
PREREQUISITE NURSING KNOWLEDGE

Parameters
Calculations
Normal Value
Body surface area (BSA)
Weight (kg) × height (cm) × 0.007184
Varies with size (range = 0.58 to 2.9 m2)
CO
HR × SV
4-8 L/min
Stroke volume (SV)
CO × 1000 ÷ HR
60-100 mL/beat
Stroke volume index (SVI)
SV ÷ BSA
30-65 mL/beat/m2
Cardiac index (CI)
CO ÷ BSA
2.5-4.5 L/min/m2
Heart rate (HR)
60-100 beats/min
Preload
Central venous pressure (CVP) or RAP
2-6 mm Hg
Left atrial pressure (LAP)
4-12 mm Hg
Pulmonary artery diastolic pressure (PADP)
5-15 mm Hg
PAOP
4-12 mm Hg
RVEDP
0-8 mm Hg
LVEDP
4-10 mm Hg
Afterload
Systemic vascular resistance (SVR)
MAP − CVP/RAP × 80 ÷ CO
900-1400 dynes/s/cm−5
SVR index (SVRI)
MAP − CVP/RAP × 80 ÷ CI
2000-2400 dynes/s/cm−5/m2
Pulmonary vascular resistance (PVR)
PAMP − PAOP × 80 ÷ CO
100-250 dynes/s/cm−5
PVR index (PVRI)
PAMP − PAOP × 80 ÷ CI
255-315 dynes/s/cm−5/m2
Systolic blood pressure
100-130 mm Hg
Contractility
Ejection fraction (EF):
Left
LVEDV × 100 ÷ SV
60%-75%
Right
RVEDV × 100 ÷ SV
45%-50%
Stroke work index:
Left
SVI (MAP − PAOP) × 0.0136
50-62 g-m/m2/beat
Right
SVI (MAP − CVP) × 0.0136
5-10 g-m/m2/beat
Pressures:
MAP
DBP + ⅓ (SBP − DBP)
70-105 mm Hg
PAMP
PADP + ⅓ (PASP − PADP)
9-16 mm Hg
 An injectate (5% dextrose in water) of a known volume (10 mL) and temperature (room or cold temperature) is injected into the right atrium (RA) through the proximal port of the PA catheter. This injectate exits in the RA, where it mixes with blood and flows through the right ventricle to the PA. A thermistor located at the tip of the PA catheter senses the change in blood temperature as the blood passes the tip of the catheter in the PA. The CO is calculated as the difference in temperatures on a time versus temperature curve.
An injectate (5% dextrose in water) of a known volume (10 mL) and temperature (room or cold temperature) is injected into the right atrium (RA) through the proximal port of the PA catheter. This injectate exits in the RA, where it mixes with blood and flows through the right ventricle to the PA. A thermistor located at the tip of the PA catheter senses the change in blood temperature as the blood passes the tip of the catheter in the PA. The CO is calculated as the difference in temperatures on a time versus temperature curve.
 A single thermistor has one inline temperature sensor near the tip of the catheter that lies in the PA when in proper position.
A single thermistor has one inline temperature sensor near the tip of the catheter that lies in the PA when in proper position.
 A dual thermistor has two inline temperature sensors, one in the right atrium/superior caval vein (immediately above the injectate port opening) and one near the tip of the catheter (same position as single thermistor). Because a temperature sensor is located in the right atrium, there is no need to enter a “correction factor” or “computation constant” into the computer to account for the loss in thermal indicator (heat) from the hub of the RA injectate port to the RA. Investigators found that the second thermistor improved accuracy when compared with Fick CO measurements and also improved precision or repeatability of CO measurements in both cold and room temperature.4,24 In one study, cold injectate had excellent precision with the standard single-thermistor PA catheter. Researchers concluded that the dual-thermistor PA catheter provided the greatest benefit in decreasing measurement variability when room temperature injections were used to measure CO.4
A dual thermistor has two inline temperature sensors, one in the right atrium/superior caval vein (immediately above the injectate port opening) and one near the tip of the catheter (same position as single thermistor). Because a temperature sensor is located in the right atrium, there is no need to enter a “correction factor” or “computation constant” into the computer to account for the loss in thermal indicator (heat) from the hub of the RA injectate port to the RA. Investigators found that the second thermistor improved accuracy when compared with Fick CO measurements and also improved precision or repeatability of CO measurements in both cold and room temperature.4,24 In one study, cold injectate had excellent precision with the standard single-thermistor PA catheter. Researchers concluded that the dual-thermistor PA catheter provided the greatest benefit in decreasing measurement variability when room temperature injections were used to measure CO.4

Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


67: Cardiac Output Measurement Techniques (Invasive)