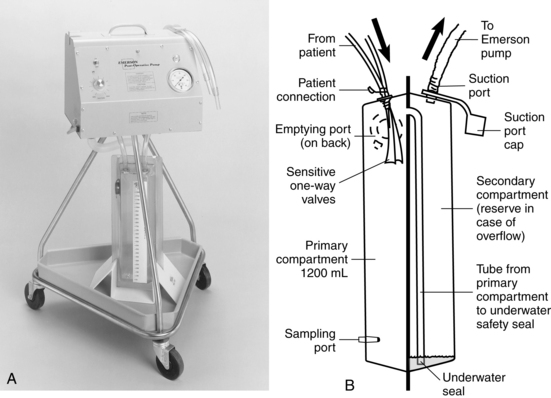
PROCEDURE 24 • Anatomy and physiology of the pulmonary system should be understood. • Normal intrapleural pressures measure approximately −4 cm H2O during expiration. At end inspiration, pressure decreases to −8 cm H2O.15 • Closed chest drainages systems are used to facilitate the evacuation of fluid, blood, and air from the pleural space, the mediastinum, or both; to restore negative pressure to the pleural space; and to promote reexpansion of a collapsed lung. • Closed chest drainage systems (CDSs) include: • Currently, guidelines recommend that a water-seal alone is safe for most patients with a pneumothorax or small air leak.2–5,8,9,20,25 However, if the pneumothorax or air leak is large, expanding, or persistent, suction is recommended.5,8,9 • The most common amount of suction pressure ranges from −10 to −20 cm H2O.1,3,8,14 High suction levels may cause persistent pleural air leaks, air stealing, lung tissue entrapment, and reexpansion pulmonary edema.14,17 • The addition of a suction source can enhance drainage when large volumes of air or fluid must be evacuated. • If clinically desirable, some disposable wet suction with traditional water-seal drainage systems can provide suction levels greater than −25 cm H2O. The suction chamber vent holes can be occluded with nonporous tape or by replacing them with the manufacturer’s special pronged vent plug and connecting directly to wall regulator suction. Suction levels must be converted from prescribed levels of cm H2O suction to mm Hg of wall suction (Table 24-1). Table 24-1 Reprinted with permission of Atrium Medical Corporation, Hudson, NH. • Some systems have accessories that may be used to convert them to an autotransfusion unit. • Some CDSs use dry suction with a traditional water-seal and either a regulator or a restricted orifice mechanism. Although water is added to the water-seal chamber, water does not need to be added to the suction chamber. Instead, the suction source (usually a wall regulator) is increased until an indicator appears. • Some CDSs are waterless, referred to as dry-dry drains, and have a one-way valve, which eliminates the need to fill any chambers (except an air-leak indicator zone, as needed). A valve opens on expiration and allows patient air to exit, then closes to prevent atmospheric air from entering during inspiration. This one-way valve feature allows the system to be used in the vertical or horizontal position without loss of the seal. These systems are safe if accidentally tipped. The amount of suction delivered is regulated with an adjustable dial. • Advantages of dry suction are ease of setup; ease of application if higher, more precise levels of suction are needed; and a quiet system. • Some clinicians suggest use of the Emerson pump (Fig. 24-2) for patients with large bronchopleural air leaks because they are high-volume, low-resistance, portable suction devices capable of handling high airflow rates.14,15 Figure 24-2 A, Emerson pump. B, Emerson disposable chest drain system. (Courtesy J.H. Emerson, Cambridge, MA.) • Tidaling, fluctuations that occur with inspiration and expiration, provides a continuous manometer of the pressure changes in the pleural space and indicates overall respiratory effort. Absence of fluctuations suggests obstruction of the drainage system from clots, contact with lung tissue, kinks, loss of subatmospheric pressure from fluid-filled dependent loops, or complete reexpansion of the lung.1,10,19 • Except for the exit vent, an airtight system is required to assist in maintaining negative pressure in the pleura and to prevent air entrapment in the pleural space. • In general, clamping of chest tubes is contraindicated. Clamping a chest tube in a patient with a pleural air leak may cause a tension pneumothorax. The few situations in which chest tubes may be clamped briefly (i.e., less than a minute) include locating the source of an air leak, replacing the chest drainage system, determining whether a patient is ready to have the chest tube removed, and during chest tube removal.1,14,15,21,26 • Disposable chest drainage unit • Suction source and regulator • Tape (1-inch), one roll, or zip ties (Parham-Martin bands)
Closed Chest Drainage System
PREREQUISITE NURSING KNOWLEDGE
 Dry suction with a traditional water-seal; dry suction with a one-way valve; wet suction with a traditional water-seal; and one-bottle, two-bottle, three-bottle, and four-bottle setups
Dry suction with a traditional water-seal; dry suction with a one-way valve; wet suction with a traditional water-seal; and one-bottle, two-bottle, three-bottle, and four-bottle setups
 Greater pressure within the chest than within the system; this requirement is accomplished by keeping the drainage unit at least 1 foot below the chest tube insertion site and the tubing free of dependent loops and obstructions,1,11,13,26 which prevents siphoning of the contents back into the pleural cavity26
Greater pressure within the chest than within the system; this requirement is accomplished by keeping the drainage unit at least 1 foot below the chest tube insertion site and the tubing free of dependent loops and obstructions,1,11,13,26 which prevents siphoning of the contents back into the pleural cavity26
 Differences in flow rates and in accuracy of delivered negative pressures noted in chest drainage systems that were not likely to be clinically important6,7
Differences in flow rates and in accuracy of delivered negative pressures noted in chest drainage systems that were not likely to be clinically important6,7
 Some systems and suction devices (e.g., Emerson pump, Cambridge, MA) contain an exit vent from the water-seal chamber that ensures the drainage unit remains vented when the suction device is off. Do not close or occlude the exit vent.19,26 With use of CDSs without an exit vent, the drainage systems should be disconnected from suction before they are turned off.19,26
Some systems and suction devices (e.g., Emerson pump, Cambridge, MA) contain an exit vent from the water-seal chamber that ensures the drainage unit remains vented when the suction device is off. Do not close or occlude the exit vent.19,26 With use of CDSs without an exit vent, the drainage systems should be disconnected from suction before they are turned off.19,26
 Some wall-mounted suction devices need control and pressure gauges to regulate and monitor for potential surges in suction levels.15,19,26
Some wall-mounted suction devices need control and pressure gauges to regulate and monitor for potential surges in suction levels.15,19,26
cm H2O
mm Hg
20
15
25
18
30
22
35
26
40
30
45
33
50
37
60
44
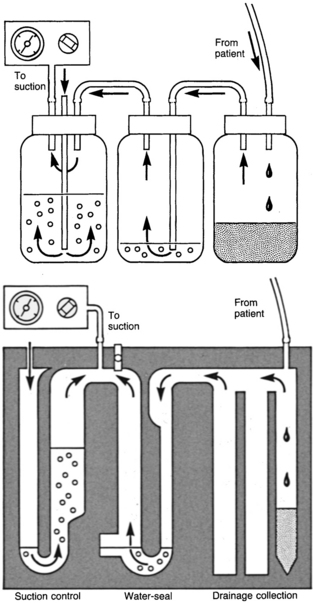
 Correlate to the three-bottle drainage system, with collection, water-seal, and suction control chambers positioned side by side in a molded plastic disposable unit (Fig. 24-1). These include the Pleur-Evac, Thora-Klex, Argyle, and Atrium systems.
Correlate to the three-bottle drainage system, with collection, water-seal, and suction control chambers positioned side by side in a molded plastic disposable unit (Fig. 24-1). These include the Pleur-Evac, Thora-Klex, Argyle, and Atrium systems.
EQUIPMENT
Disposable Setup (Wet and Dry Systems)
Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


24: Closed Chest Drainage System