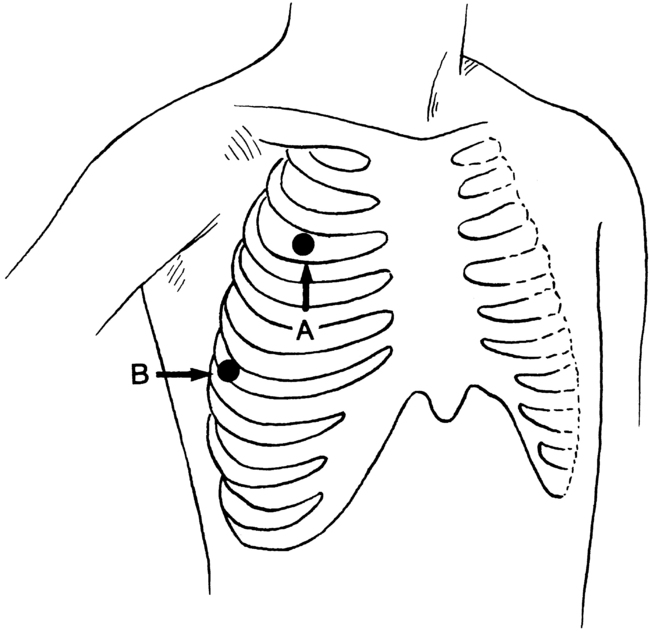
PROCEDURE 20 • The thoracic cavity, in normal conditions, is a closed airspace. Any disruption results in the loss of negative pressure within the intrapleural space. Air or fluid that enters the space competes with the lung, resulting in collapse of the lung. Associated conditions are the result of disease, injury, surgery, or iatrogenic causes. • Chest tubes are sterile flexible vinyl or silicone nonthrombogenic catheters approximately 20 inches (51 cm) long, varying in size from 12F to 40F. The size of the tube placed is determined by the condition. Chest tubes inserted for traumatic hemopneumothorax or hemothorax (blood) should be large (36F to 40F). Medium tubes (24F to 36F) should be used for fluid accumulation (pleural effusions). Tubes inserted for pneumothorax (air) should be small (12F to 24F).2 • Indications for chest tube insertion include the following: • A pneumothorax may be classified as an open, closed, or tension pneumothorax. • Lung that is densely adherent to the chest wall throughout the hemithorax is an absolute contraindication to chest tube therapy.4 • Use of chest tubes in patients with multiple adhesions, giant blebs, or coagulopathies is carefully considered; however, these relative contraindications are superseded by the need to reexpand the lung. When possible, any coagulopathy or platelet defect should be corrected before chest tube insertion. The differential diagnosis between a pneumothorax and bullous disease necessitates careful radiologic assessment.4 • The tube size and insertion site selected for the chest tube are determined by the indication.4 If draining air, the tube is placed near the apex of the lung (second intercostal space); if draining fluid, the tube is placed near the base of the lung (fourth or fifth intercostal space; Fig. 20-1). Figure 20-1 Standard sites for tube thoracostomy. A, The second intercostal space, midclavicular line. B, The fourth or fifth intercostal space, midaxillary line. Most clinicians prefer midaxillary line placement for all chest tubes, regardless of pathology. Placement of the tube too far posteriorly does not allow the patient to lie down comfortably. (From Roberts JR, Hedges JR, editors: Clinicals in emergency medicine, ed 4, Philadelphia, 2004, Saunders.) • Antiseptic solution or swab packets • Caps, masks, sterile gloves, gowns, drapes • Protective eyewear (goggles) • Local anesthetic: 1% lidocaine solution (without epinephrine) • Tube thoracotomy insertion tray
![]() Chest Tube Placement (Perform)
Chest Tube Placement (Perform)
PREREQUISITE NURSING KNOWLEDGE
 Pneumothorax (collection of air in the pleural space)
Pneumothorax (collection of air in the pleural space)
 Hemothorax (collection of blood)
Hemothorax (collection of blood)
 Hemopneumothorax (accumulation of air and blood in the pleural space)
Hemopneumothorax (accumulation of air and blood in the pleural space)
 Thoracotomy (e.g., open heart surgery, pneumonectomy)
Thoracotomy (e.g., open heart surgery, pneumonectomy)
 Pyothorax or empyema (collection of pus)
Pyothorax or empyema (collection of pus)
 Chylothorax (collection of chyle from the thoracic duct)
Chylothorax (collection of chyle from the thoracic duct)
 Cholothorax (collection of fluid containing bile)
Cholothorax (collection of fluid containing bile)
 Hydrothorax (collection of noninflammatory serous fluid)
Hydrothorax (collection of noninflammatory serous fluid)
 Open pneumothorax: The chest wall and the pleural space are penetrated, which allows air to enter the pleural space, as in penetrating injury or trauma, surgical incision in the thoracic cavity (i.e., thoracotomy), or complication of surgical treatment (e.g., unintentional puncture during invasive procedures, such as thoracentesis or central venous catheter insertion).
Open pneumothorax: The chest wall and the pleural space are penetrated, which allows air to enter the pleural space, as in penetrating injury or trauma, surgical incision in the thoracic cavity (i.e., thoracotomy), or complication of surgical treatment (e.g., unintentional puncture during invasive procedures, such as thoracentesis or central venous catheter insertion).
 Closed pneumothorax: The pleural space is penetrated, but the chest wall is intact, which allows air to enter the pleural space from within the lung, as in spontaneous pneumothorax. A closed pneumothorax occurs without apparent injury and often is seen in individuals with chronic lung disorders (e.g., emphysema, cystic fibrosis, tuberculosis, necrotizing pneumonia); in young, tall men who have a greater than normal height-to-width chest ratio; after blunt traumatic injury; or iatrogenically, occurring as a complication of medical treatment (e.g., intermittent positive-pressure breathing [IPPB], mechanical ventilation with positive end-expiratory pressure [PEEP]).
Closed pneumothorax: The pleural space is penetrated, but the chest wall is intact, which allows air to enter the pleural space from within the lung, as in spontaneous pneumothorax. A closed pneumothorax occurs without apparent injury and often is seen in individuals with chronic lung disorders (e.g., emphysema, cystic fibrosis, tuberculosis, necrotizing pneumonia); in young, tall men who have a greater than normal height-to-width chest ratio; after blunt traumatic injury; or iatrogenically, occurring as a complication of medical treatment (e.g., intermittent positive-pressure breathing [IPPB], mechanical ventilation with positive end-expiratory pressure [PEEP]).
 Special applications: Chest tubes can be used to instill anesthetic solutions and sclerosing agents.
Special applications: Chest tubes can be used to instill anesthetic solutions and sclerosing agents.
 When the tube is in place, the tube is sutured to the skin to prevent displacement, and an occlusive dressing is applied (see Fig. 21-1). The chest tube also is connected to a chest drainage system (see Procedure 24) to remove air and fluid from the pleural space, which facilitates reexpansion of the collapsed lung. All connection points are secured with tape or zip ties (Parham-Martin bands) to ensure that the system remains airtight (see Fig. 21-2).
When the tube is in place, the tube is sutured to the skin to prevent displacement, and an occlusive dressing is applied (see Fig. 21-1). The chest tube also is connected to a chest drainage system (see Procedure 24) to remove air and fluid from the pleural space, which facilitates reexpansion of the collapsed lung. All connection points are secured with tape or zip ties (Parham-Martin bands) to ensure that the system remains airtight (see Fig. 21-2).
 Mediastinal tubes generally are placed in the operating room by a surgeon after cardiac surgery.
Mediastinal tubes generally are placed in the operating room by a surgeon after cardiac surgery.
EQUIPMENT
Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


20: Chest Tube Placement (Perform)









