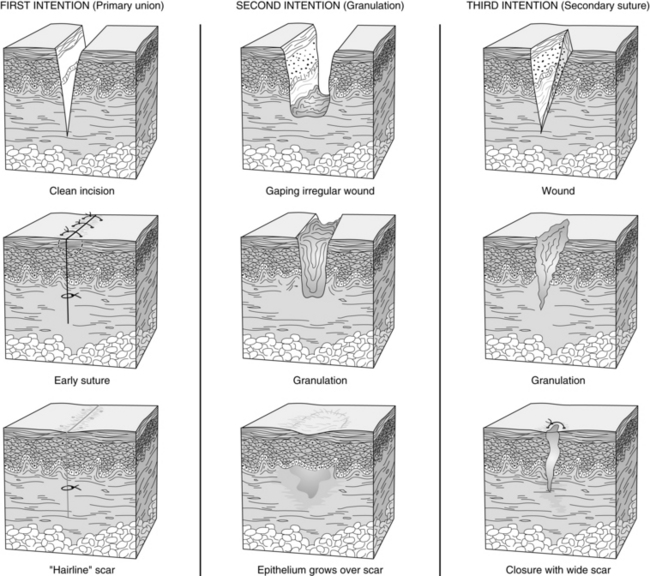
PROCEDURE 126 • Goals of wound care must be clearly outlined so that proper wound care products are used. • Wound care products should be matched to the patient and wound conditions. Although no specific dressing is considered superior to others,9,13 properties of dressing products are different and should be assessed relative to wound treatment goals.2,9 • Wounds heal by primary, secondary, or tertiary intention (Fig. 126-1). • Clean, moist wound beds allow for effective wound healing under the support of a dressing. • Wound cleansing should be accomplished with minimal chemical or mechanical trauma. • Wound infections delay wound healing. Wound cultures (obtained before antibiotic therapy) may isolate organisms and differentiate between colonization and active infection.
Cleaning, Irrigating, Culturing, and Dressing an Open Wound
PREREQUISITE NURSING KNOWLEDGE
 Dressings may be categorized as semiocclusive or occlusive. Semiocclusive dressings are semipermeable to gases (O2, CO2, moisture) and are impermeable to liquids; they provide the moist wound healing environment that optimizes wound healing. Occlusive dressings lack permeability to gases and liquids.
Dressings may be categorized as semiocclusive or occlusive. Semiocclusive dressings are semipermeable to gases (O2, CO2, moisture) and are impermeable to liquids; they provide the moist wound healing environment that optimizes wound healing. Occlusive dressings lack permeability to gases and liquids.
 Normal wound healing is often described as a progressive process that involves three overlapping phases: inflammation, proliferation, and maturation. The inflammatory phase is marked for hemostasis, increased vasodilation, and migration of neutrophils and macrophages to the area. The proliferation phase begins 2 to 4 days after injury and is the healing phase of the wound process in which epithelialization, angiogenesis, and collagen synthesis predominate.8,9 The maturation phase involves the body remodeling collagen fiber and increasing tissue tensile strength.8,9
Normal wound healing is often described as a progressive process that involves three overlapping phases: inflammation, proliferation, and maturation. The inflammatory phase is marked for hemostasis, increased vasodilation, and migration of neutrophils and macrophages to the area. The proliferation phase begins 2 to 4 days after injury and is the healing phase of the wound process in which epithelialization, angiogenesis, and collagen synthesis predominate.8,9 The maturation phase involves the body remodeling collagen fiber and increasing tissue tensile strength.8,9
 Openly granulating wounds heal more slowly, may result in drying of granulating tissue and tissue death, and may be more painful for the patient.
Openly granulating wounds heal more slowly, may result in drying of granulating tissue and tissue death, and may be more painful for the patient.
 The presence of exudate is not synonymous with infection but is the natural result of the inflammatory response to maintain moisture and allow movement and replication of epithelial cells necessary for healing. A change in volume, color, or consistency of exudate may indicate impending infection.2,4,12
The presence of exudate is not synonymous with infection but is the natural result of the inflammatory response to maintain moisture and allow movement and replication of epithelial cells necessary for healing. A change in volume, color, or consistency of exudate may indicate impending infection.2,4,12
 Cytotoxic cleaning agents (i.e., chlorhexidine, iodine, hydrogen peroxide) should be limited because they can delay healing.1,4,9,12
Cytotoxic cleaning agents (i.e., chlorhexidine, iodine, hydrogen peroxide) should be limited because they can delay healing.1,4,9,12
 Wound cleaning solutions should be pH neutral.
Wound cleaning solutions should be pH neutral.
 Normal saline (NS) solution is the cleaning agent of choice; however, tap water is safe and effective for cleaning of most acute and chronic wounds.1,5,14
Normal saline (NS) solution is the cleaning agent of choice; however, tap water is safe and effective for cleaning of most acute and chronic wounds.1,5,14
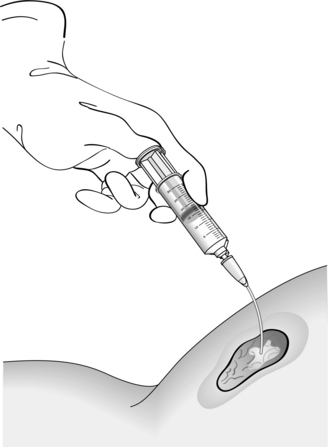
 The cleaning solution must be delivered with enough force to physically loosen foreign materials and bacteria without injuring the tissue. Effective wound cleaning is best achieved when solution is delivered at 8 to 13 psi (Fig. 126-2). A 35-mL syringe attached to an 18-gauge angiocatheter tip only delivers fluid at 8 psi. A 12-mL syringe with a 22-gauge angiocatheter tip provides 13 psi. (Increasing syringe size decreases the pressure of the stream, and increasing the bore of the catheter tip increases the pressure.) Pressures greater than 15 psi may actually force bacteria and debris deeper into the wound bed.2,8,9,12
The cleaning solution must be delivered with enough force to physically loosen foreign materials and bacteria without injuring the tissue. Effective wound cleaning is best achieved when solution is delivered at 8 to 13 psi (Fig. 126-2). A 35-mL syringe attached to an 18-gauge angiocatheter tip only delivers fluid at 8 psi. A 12-mL syringe with a 22-gauge angiocatheter tip provides 13 psi. (Increasing syringe size decreases the pressure of the stream, and increasing the bore of the catheter tip increases the pressure.) Pressures greater than 15 psi may actually force bacteria and debris deeper into the wound bed.2,8,9,12
 Wound contamination is the presence of bacteria on the wound surface that are not actively multiplying. Signs and symptoms of infection are not present, and healing is not impaired.4,12
Wound contamination is the presence of bacteria on the wound surface that are not actively multiplying. Signs and symptoms of infection are not present, and healing is not impaired.4,12
 Wound infection is present if organisms are present at 105 colony-forming units per milliliter (103 for virulent organisms like β-hemolytic strep4) in conjunction with clinical findings such as erythema, edema, pain, purulence, fever, and leukocytosis.
Wound infection is present if organisms are present at 105 colony-forming units per milliliter (103 for virulent organisms like β-hemolytic strep4) in conjunction with clinical findings such as erythema, edema, pain, purulence, fever, and leukocytosis.Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


126: Cleaning, Irrigating, Culturing, and Dressing an Open Wound