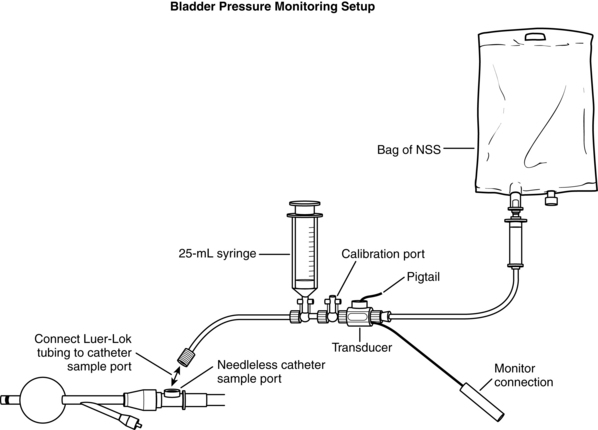
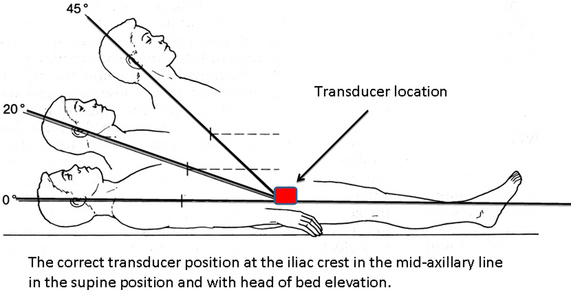
PROCEDURE 106 Intraabdominal hypertension and abdominal compartment syndrome occur when the abdominal contents expand in excess of the capacity of the abdominal cavity, compromising abdominal organ perfusion and resulting in organ dysfunction or failure and associated mortality.3,5,9,13,14,17,20,23,25 • Understanding of gastrointestinal anatomy and physiology is necessary. • Knowledge of aseptic technique is essential. • Intraabdominal hypertension (IAH) and abdominal compartment syndrome (ACS) occur when the abdominal contents expand in excess of the capacity of the abdominal cavity, compromising abdominal organ perfusion and resulting in organ dysfunction or failure and associated mortality.3,5,9,13,14,17,20,23,25 • Four major categories of risk are associated with the development of IAH and ACS (Table 106-1).3,17 They include: Table 106-1 Patients at Risk for Development of Intraabdominal Hypertension and Abdominal Compartment Syndrome3,17 (Levels C, D, E*) *Level C: Qualitative studies, descriptive or correlational studies, integrative reviews, systematic reviews, or randomized controlled trials with inconsistent results *Level D: Peer-reviewed, professional organizational standards with clinical studies to support recommendations *Level E: Multiple case reports, theory-based evidence from expert opinions, or peer-reviewed professional organizational standards without clinical studies to support recommendations • IAH is defined as a sustained or repeated pathologic elevation of intraabdominal pressure (IAP) to more than or equal to 12 mm Hg.3,17 • IAH is graded by severity3,17: • ACS is defined as IAP more than or equal to 20 mm Hg that is associated with new organ dysfunction or failure.1,3,17,20,21,25 ACS is categorized into three types3,12,17: • Both IAH and ACS may compromise perfusion to the visceral organs represented by the parameter: abdominal perfusion pressure (APP).3,6–8,17 APP is derived as: • APP should be maintained at more than 50 to 60 mm Hg to maintain adequate perfusion to the abdominal organs and reduce the chance of organ dysfunction.3,6,7,17 • Measurement of bladder pressure via an indwelling urinary bladder catheter is considered the reference standard for the measurement of IAP and may be performed with equipment readily available in the critical care environment (Fig. 106-1).2,3,8,15,17,22 Commercially prepared kits designed for measurement of IAP are also available and may provide advantages in efficiency, standardization of measurement technique, and data reproducibility. Instructions for specific setup and operation of commercially prepared devices are provided by the manufacturer. Note that regardless of the device used, a standardized procedure for measurement should be used to prevent measurement variability between practitioners.12,15,22 • The bladder acts as a passive reservoir and accurately reflects IAP when intravesicular volumes of 25 mL or less are used. Larger volumes previously suggested (50 to 100 mL) are not necessary and may in fact overdistend the bladder, falsely elevating measured bladder pressure (IAP).3,11,18 • Normal IAP is 0 mm Hg and may even be subatmospheric. In patients who are critically ill, it may rise to 5 to 7 mm Hg.3,17 • IAP should be measured with the patient in the supine position. The transducer should be leveled or zeroed at the iliac crest in the midaxillary line (Fig. 106-2).2,3,17,24 Figure 106-2 Correct position of the transducer for bladder pressure measurement. (Illustration by John J. Gallagher.) • IAP should be measured at end expiration. Wait an appropriate time (10 to 60 seconds) after saline solution instillation to allow for equilibration of the monitor to a steady state pressure reading.3,17 • IAP should be expressed in millimeters of mercury (mm Hg; 1 mm Hg = 1.36 cm H2O).3,17 • Serial monitoring of bladder pressures is useful in detection of the onset of IAH and the progression to the more severe condition of ACS. Recommendations are that measurements be repeated every 2 to 4 hours in patients with IAP more than or equal to 12 mm Hg so a trend may be established and increases in pressure are detected.3,17 • Bladder pressure measurement may be contraindicated in certain conditions, such as bladder trauma, bladder surgery, and neurogenic bladder. Risks and benefits of measurement should be discussed with the physician before the procedure is performed in these patients. • In patients who do not have a urinary catheter in place, the risks and benefits of catheter placement for the purpose of bladder pressure measurement should be considered.
Intraabdominal Pressure Monitoring
PREREQUISITE NURSING KNOWLEDGE
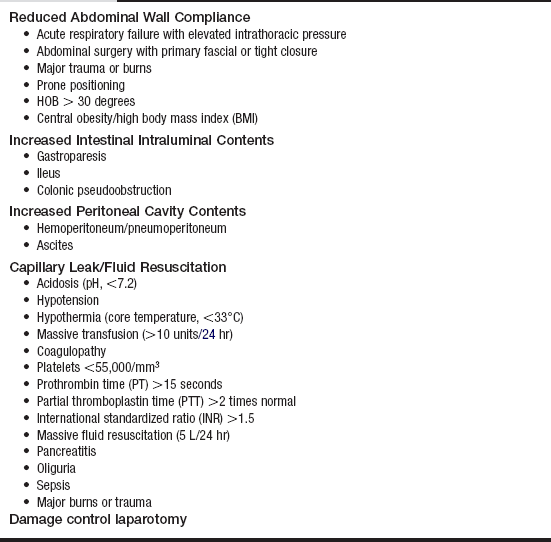
 Diminished abdominal wall compliance
Diminished abdominal wall compliance
 Increased intestinal intraluminal contents
Increased intestinal intraluminal contents
 Increased peritoneal cavity contents
Increased peritoneal cavity contents
 Capillary leakage into the bowel wall and mesentery/fluid resuscitation
Capillary leakage into the bowel wall and mesentery/fluid resuscitation


Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


106: Intraabdominal Pressure Monitoring