Fig. 4.1
ECG in normal sinus rhythm; with usual setting (paper speed 25 mm/s) 1 mm equals with 40 ms interval
Each QRS complex is preceded by a P wave with a rate between 60 and 100 bpm with the exception of newborns and infants in whom normal HR is higher (150–230 bpm in newborn) [7].
P wave is positive in leads I–II and aVL–aVF and in precordial leads from V2–3 to V6, is negative in aVR and can be negative in III, and is biphasic in V1–V2; P wave lasts 120 ms (3 mm).
Between P wave and QRS complex, there is an isoelectric region (flat line on ECG) which lasts 120–200 ms: the PR interval.
QRS is narrow (<110 ms).
While approaching a patient with symptomatic supraventricular tachycardia, physicians must evaluate the patient’s clinical status to identify potential reversible causes of tachycardia and to assess the degree of instability and understand if it is related to the tachycardia itself.
Arterial blood pressure, oxygen saturation, electrolyte, and hemoglobin must be evaluated; ECG monitoring and intravenous access must be established.
If possible a 12-lead ECG should be performed during the arrhythmia (and after its interruption) [2].
4.1.1 Patients in Unstable Condition
If the patient demonstrates rate-related cardiovascular compromise with signs and symptoms such as acute altered mental status, ischemic chest discomfort, acute heart failure, hypotension, or other signs of shock suspected to be due to a tachyarrhythmia, proceed to immediate synchronized electrical cardioversion (after sedation of the patient if conscious); provide oxygen if oxygen saturation is below 94 % [2]:
Narrow regular tachycardia → biphasic synchronized direct current shock 50–100 J
Narrow irregular tachycardia → biphasic synchronized direct current shock 120–200 J
Wide regular tachycardia → biphasic synchronized direct current shock 100 J
Wide irregular tachycardia → biphasic NOT synchronized direct current shock 200 J
If there’s no response to the first shock, it may be reasonable to increase the dose in a stepwise fashion.
Cardioversion with monophasic waveforms should begin at 200 J and increase in stepwise fashion if not successful [2].
In newborn, use 0.5 → 2 J/kg [3].
Heparin (low molecular weight or unfractionated heparin) should be administered before cardioversion in case of atrial flutter or atrial tachycardia and after it, depending on patients’ features (CHA2DS2VASc – HAS BLED) [8].
4.1.2 Patients in Stable Condition
The initial assessment should:
1.
Distinguish between narrow and wide complex tachycardia.
2.
Determine whether the rhythm is irregular or regular (<10 % of variation in cycle length).
3.
Consider the rapidity of onset.
4.
Identify sinus tachycardia (the theoretical upper rate is 220bpm minus the patient’s age in years).
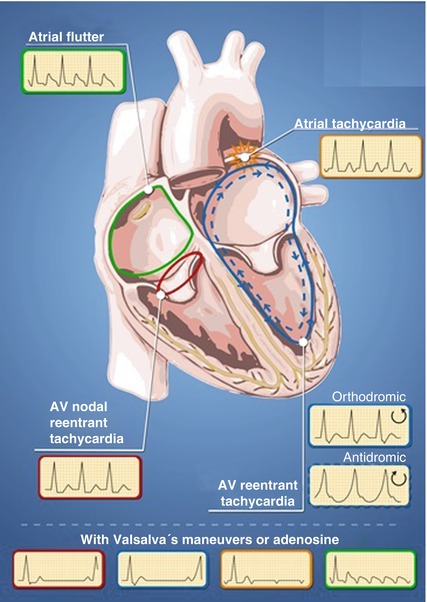
Supraventricular tachycardias have narrow QRS in 90 % of cases. Wide QRS complex could be due to pre-excitation through an accessory pathway or to bundle-branch block or to pacemaker stimulation. Previous ECG and ECG after termination of tachycardia can help to make the diagnosis.
While considering the patient’s history, the clinician should assess the duration and frequency of episodes, the mode of onset, and possible triggers (including the intake of alcohol, caffeine or other drugs) as well as previous cardiac or other diseases or previous ECGs.
Supraventricular tachycardias have a sudden onset and termination, in contrast to sinus tachycardias or atrial tachycardias, which accelerate and decelerate gradually; however, some patients do not perceive the sudden onset of supraventricular tachycardia; furthermore, sometimes, they describe sudden onset and gradual offset due to reactive sinus tachycardia after termination of paroxysmal SVT. It may be misdiagnosed as panic disorder [5, 9].
Physical examination during episodes may reveal the “frog sign” which is a prominent jugular venous A waves due to atrial contraction against the closed tricuspid valve. After sinus rhythm is restored, physical examination is usually normal, but a careful examination is warranted to rule out evidence of structural heart disease [11, 12].
4.1.3 Management
4.1.3.1 Narrow QRS
If narrow QRS is present, atrioventricular conduction is certainly entirely through atrioventricular node. That’s why maneuvers that increase vagal tone and block atrioventricular conduction are safe: they can interrupt tachycardias depending on AV node conduction (TRNAV or orthodromic TRAV) and can slow down those which don’t depend on AV node conduction (atrial flutter or atrial fibrillation). They also interrupt focal tachycardia due to enhanced automaticity.
Physicians have these possibilities:
Vagal maneuvers (Valsalva, carotid sinus massage, facial immersion in cold water, and bearing down). The efficacy is about 25 % [13]. Remember that carotid sinus massage is contraindicated in case of carotid stenosis.
Adenosine: very short-acting endogenous nucleotide (<10 s). It blocks atrioventricular nodal conduction and terminates most of atrioventricular nodal reentrant tachycardias and atrioventricular reciprocating tachycardias as well as up to 80 % of atrial tachycardias [14–16]. Since it may also have proarrhythmic effect (atrial fibrillation in 12 % of patients), it must be administered under ECG monitoring with an accessible defibrillator.
Common side effects include chest tightness, flushing, and a sense of dread. Avoid in asthmatic patients since it can produce bronchospasm; patients with autonomic failure and with cardiac transplant or patient chronically treated with antiarrhythmic drugs are more sensitive to adenosine [17]; that’s why doses must be halved.
Way of administration and doses: 0.1–0.2 mg/kg (usually 6–12 mg) through peripheral vein; start with 6 mg in a rapid flush immediately followed by 20 ml of saline flush. If there is no effect, try again with 12 mg. Same dose for newborn.
Verapamil -diltiazem: Intravenous verapamil and diltiazem are effective in interrupting tachycardias or can slow down AV conduction, but can cause hypotension thus are not recommended as first choice in the emergency setting [18]. They are contraindicated in heart failure and in newborn because of risk of cardiac arrest or atrioventricular dissociation [3, 19].
Electrical cardioversion: best choice for atrial fibrillation and atrial flutter (typical o atypical) with onset within 48 h or in anticoagulated patients [8]. Biphasic synchronized shock (50 → 200 J; 0.5 → 2 J/kg in infants) is recommended in sedated patient. Before cardioversion, a heparin bolus is recommended in all patients not yet anticoagulated. If there is no efficacy or there is arrhythmia recurrence, pharmacological therapy can be added.
Remember that:
Sinus tachycardia is usually reactive to other causes so identification and treatment of them are required. No specific drug treatment is usually necessary.
Atrial fibrillation and atrial flutter can give rise to endocardial thrombus which can cause stroke or thromboembolism: the risk is higher after 48 h of persistent tachycardia and in patients with some specific features (CHA2DS2VASc > 1). For this reason, anticoagulation (for at leat 3 weeks) is mandatory before cardioversion (or, in alternative, perform trans-esophageous echo to rule out intracardiac thrombi); in case of arrhythmias lasting more than 48 h or non-datable; nevertheless, heparin administration before cardioversion is preferable in all patients. For more details, see specific guidelines [16, 19–21].
Patients with uncomplicated tachycardias and without cardiomyopathy can be discharged after sinus rhythm restoration; cardiological evaluation can be postponed.
Sodium channel blockers increase both pacing threshold and the energy required to defibrillation [22, 23].
Being genetic setting unknown, the effect of an antiarrhythmic drug given for the first time is never predictable. That’s why administration of antiarrhythmic medications for the first time must be done under ECG monitoring lasting for at least the drug’s half-time; after discharge, if chronic therapy is set up, ECG must be checked at the steady state (five half-times) (Fig. 4.2).
4.1.3.2 Wide QRS
Wide QRS can be due to preexisting or frequency-dependent bundle-branch block or to conduction over an accessory pathway. Nevertheless, the majority of wide QRS complex tachycardia has ventricular origin. If the patient is in stable hemodynamic condition, it is better to refer him/her to a specialist for diagnosis and treatment.
4.2 What Cardiologists Should Know
Cardiologist should evaluate all patients with hemodynamic instability related to tachycardias after their stabilization with cardioversion in order to exclude or confirm the presence of cardiomyopathy, to decide the best medical treatment, and to decide for hospitalization or discharge and follow-up.
Non-urgent cardiological examination within few weeks can be reserved to uncomplicated tachycardias, in absence of cardiomyopathy, especially in case of preexisting diagnosis.
Cardiologist should know mechanisms underlying arrhythmias and modality of action of antiarrhythmic drugs in order to choose and combine them, to maximize efficacy and minimize proarrhythmic and side effects [22, 23], and to remove precipitating features as ischemia and electrolyte imbalance.
For this reason, the next part of the chapter is dedicated to pharmacology of antiarrhythmic drugs and basic electrophysiology.
At the end of the chapter, a scheme of therapies for each arrhythmia is provided.
4.2.1 Basic Electrophysiologic Principles
Every heart contraction is driven by inversion of cell potential from negative to positive. At the cell membrane site, this potential variation from negative to positive (depolarization) and back to negative (repolarization) is called action potential (AP). This is possible thanks to the activation in sequence of different channels driving ion currents (I) inward and outward the cell; every channel is designed to allow passage of its own specific ion and to do it only during a specific phase of AP (some channels open only at negative potential, other at positive). Potassium (K+) is mainly inside the cell, while sodium (Na+) is outside and calcium (Ca++) is both outside and stored inside the cell; sodium and calcium are linked to one another. To generate cell depolarization, a specific potential threshold must be reached.
Action potential has been divided in five phases:
0 → Depolarization
1 → Fast repolarization
2 → Plateau
3 → Terminal repolarization
4 → Resting
During the first phase of action potential, cell membrane is depolarized, and no external stimulus can modify it (absolute refractoriness); during repolarization, external factors can excite the cell with “extra-AP” (relative refractoriness).
Propagation of action potential from a cell to another is called conduction and is characterized by a speed and a safety factor.
Action potential has different morphologies in different tissues (sinus node, AV node, atrioventricular cells). This is due to different kinds of channels and explains the heterogeneous effects of antiarrhythmic drugs on each cardiac tissue.
For example, AV node cell depolarization is mainly calcium mediated, while atrial and ventricular depolarization is sodium mediated; automaticity of sinus node is due to specific channels (HCN) which are permeable to both sodium and potassium and open only at very negative potentials (hyperpolarization).
4.2.2 Mechanisms of Arrhythmias
Arrhythmias are divided into focal and reentrant.
4.2.2.1 Focal
Focal supraventricular tachycardias are defined as an activation starting rhythmically from a small area in atria or AV junction and spreading out centrifugally. Focus can be single or multiple. Mechanism underlying focal tachycardias is automaticity, triggered activity, and micro-reentrant.
Get Clinical Tree app for offline access

Triggered activity: abnormal fluctuations of action potential occurring after or during the repolarization (phase 2–3 or 4 of action potential), which are able to depolarize cell membrane to the depolarization threshold; differently from automatic foci, they are linked to the previous action potential. Three kinds of triggered activities are known (Fig. 4.3):
Fig. 4.3
Effects of early after depolarization (EAD), delayed after depolarization (DAD), and automaticity on action potential
(a)
Early after depolarization (EAD) → occurring during repolarization (phases 2–3 of action potential), due to decreased potassium conductance (typically bradycardia, hypokalemia, or class III antiarrhythmic drugs). They are suppressed by factors that increase potassium outward current (overdrive – tachycardias, K+ channels activators) or suppress sodium/calcium inward currents (e.g., magnesium).
(b)
Delayed after depolarization (DAD) → occurring during diastolic phase of action potential (phase 4) as consequence of Ca++ intracellular overload and Ca++ sparks due to increase of INa (ischemia or digoxin intoxication) or cAMP after beta-stimulation (tachycardia). They are suppressed by beta-blockers, calcium channel blockers, vagal stimulation, or adenosine.
(c)
Enhanced automaticity: positive ionic influx (mostly inward calcium current) during phase 4 (diastolic) depolarization (normal automaticity is driven by sodium current while pathological by calcium). Beta-adrenergic stimulation enhances calcium current and facilitates these arrhythmias. Automatic tachycardias are the most common kind of focal arrhythmias and are characterized by sudden onset with a “warm-up” period. Vagal stimulation, adenosine, beta-blockers, or calcium channel blockers may suppress them.Related posts:
 Management of Arrhythmic Patients in the Emergency Department: General Principles
Management of Arrhythmic Patients in the Emergency Department: General Principles
 Syncope: First Evaluation and Management in the Emergency Department
Acute Management of Patients with Arrhythmias and Non-cardiac Diseases: Metabolite Disorders and Ion Disturbances
Syncope: First Evaluation and Management in the Emergency Department
Acute Management of Patients with Arrhythmias and Non-cardiac Diseases: Metabolite Disorders and Ion Disturbances
 Acute Management of Arrhythmias in Patients with Channelopathies
Acute Management of Arrhythmias in Patients with Channelopathies
 Atrial Flutter and Fibrillation in the Emergency Setting
Atrial Flutter and Fibrillation in the Emergency Setting
 Wide QRS Complex Tachycardia in the Emergency Setting
Wide QRS Complex Tachycardia in the Emergency Setting

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

