36 Zygapophysial Joint Pain
Procedures for Diagnosis and Treatment
Zygapophysial joint (ZJ) pain stems from synovial ZJs, which are formed by adjacent articular processes (or apophyses) of the vertebrae. In the past, these joints were commonly called “facet joints” but that term is inappropriate because most synovial joints of the body (such as those of the elbows, wrists, and hands) have facets. The term “zygapophysial joints” is the correct name for the spinal synovial joints in current anatomic nomenclature.1
The phenomenon of lumbar ZJ pain was first mooted in 19112 and gradually gained acceptance,3,4 but since the 1930s when intervertebral disc surgery became feasible as a treatment for spinal pain, ZJ pain has been overshadowed in the minds of many by disc pain. Cervical ZJ pain has been established scientifically for only the last few decades.5,6 Over that time, a great deal of scientific research has been done and a considerable body of literature has been produced. ZJ pain has also generated considerable interest in clinical, funding, and medicolegal fields. Controversies have arisen about the etiology of ZJ pain and about the reliability, validity, and effectiveness of methods used to address it. Against that background, it is important for clinicians to appreciate the methods available for the diagnosis and treatment of ZJ pain and the scientific evidence on which they are based.
Zygapophysial Joints
Anatomy
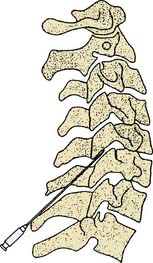
The ZJs are paired synovial joints that link the posterior elements of the spine from the C2-3 level down to the lowest spinal motion segment, L5-S1.7 At each of these cervical, thoracic, and lumbar spinal levels, the two adjacent vertebrae are linked by three articulations: at the front is a synarthrodial interbody joint linking the anterior spinal elements (the vertebral bodies) and at the back are two diarthrodial (synovial) ZJs, one on the left and one on the right, linking the posterior spinal elements (the neural arches of the vertebrae that enclose the spinal canal8) as indicated in Figure 36-1.
A ZJ is made up of two bony processes or apophyses, a superior and an inferior articular process, each of which has an articular surface (or facet) lined with hyaline cartilage about 1 to 2 mm. thick.9 Under the cartilage is a thickened layer of the subchondral bone. The joint surfaces are enveloped by a collagenous articular capsule which has superior and inferior capsular recesses above and below the main joint space.10,11 The joint space, including the recesses, is typically of about 1 mL in volume.12 The capsule is lined internally with synovial membrane, which with the cartilaginous joint surfaces, encloses the joint space. Within the joint space but outside the synovial membrane there are often intraarticular inclusions, the most common being adipose tissue pads and fibroadipose meniscoids.13 The morphologic features of specific cervical, thoracic and lumbar joints will be addressed in the following section on biomechanics and the sections on the various interventional procedures.
The nerve supply of the ZJs is via the medial branches of the dorsal rami of the spinal nerves.5,14,15 More specifically, the ZJs are supplied by articular branches of the medial branches; these articular branches are simply groups of medial branch dendrites that join the main trunks of their respective medial branches in the posterior parts of their courses. The joint capsules are richly innervated by sensory afferent fibers (first order neurons) which transmit neural impulses from each joint via the medial branch nerves to their cell bodies in the dorsal root ganglia and then on to synapse with second order neurons in the dorsal horn of the spinal cord; from there impulses are transmitted via central pathways to the sensory cortex.
Most ZJs are supplied by two medial branches, those of the spinal nerves above and below the joint. In the cervical spine from C3-4 down the two medial branches that supply each joint are those numbered accordingly. For example the C5-6 ZJ is supplied by the C5 and C6 medial branches. Because there are eight cervical spinal nerves, the C7-T1 ZJ is supplied by the C7 and C8 medial branches. Then from T1-2 downward the medial branches that supply the thoracic and lumbar ZJs are numbered one less than the corresponding joint. Thus, for example, the T1-2 ZJ is supplied by the C8 and T1 medial branches, the T8-9 ZJ by the T7 and T8 medial branches and the L4-5 ZJ by the L3 and L4 medial branches. To reduce confusion in the designation of ZJs and medial branches the International Spine Intervention Society (ISIS), which sets standards of practice and publishes practice guidelines for spinal interventions, has established a convention for denoting joints by the use of a hyphen (e.g., the left L4-5 ZJ) and denoting nerves by the use of a comma (e.g., the L3,4 medial branches).16 This convention is recommended for use in all written records.
The medial branches lie close to the bone of the joint partners and are mostly bound down to it by fascia. Over the medial branches are the deep layers of the paraspinal muscles. The anatomic relationships of the nerves to the bones vary with the morphology of the cervical, thoracic, and lumbar regions. Generally speaking, the cervical medial branches run obliquely across the waists of the articular pillars of the joint partners to the intervertebral foramina where they join the dorsal rami. The thoracic and lumbar medial branches run obliquely across the articular pillars and over the tops of the transverse processes of their vertebrae. The courses of the medial branches will be considered in more detail in the later sections on medial branch blocks.
The facets of the ZJs have surface areas of about 100-160 square mm. Their surfaces are curved and their anatomic orientations vary with the morphology of the cervical, thoracic, and lumbar regions. The orientations and their functional significance in each part of the spine will be considered in the section on biomechanics. As stated above, the joints properly termed zygapophysial are those of the twenty-three spinal motion segments from C2-3 down to L5-S1. Above C2-3 are the two uppermost spinal segments designated C0-1 and C1-2. The anatomy of those segments is specialized and their synovial joints that correspond to the ZJs lower down are designated by their anatomic joint partners, as the atlantooccipital joints (at C0-1) and the lateral atlantoaxial joints (at C1-2). These joints are also paired, with a left and a right joint at each level. The atlantooccipital joints involve two superior articular processes of the C1 vertebra (also called the atlas) which have concave facets that articulate with the convex facets of the occipital condyles of the base of the skull. The atlantoaxial joints, between the C1 vertebra (or atlas) and the C2 vertebra (the axis) are actually three in number. Anteriorly is the median atlantoaxial joint, a single synovial trochoid joint in which the odontoid process (or dens) of the axis rotates between the anterior arch of the atlas (in front of it) and the cruciate ligament (behind it). The lateral atlantoaxial joints (LAAJs) are paired synovial joints, one on each side, between the inferior articular processes of the atlas and the superior articular processes of the axis.17
The nerve supplies of the atlantooccipital and LAAJs are different from those of the ZJs. The atlantooccipital joints are supplied by the C1 nerve roots via their ventral rami, which follow curved courses around the outside of the arch of the atlas on each side.17 The LAAJs are supplied by the C2 spinal nerves, each of which lies immediately behind the LAAJ on that side bound to its inferior joint partner (the superior articular process of the axis) by fascia.17 The C2 spinal nerve divides behind the LAAJ into its ventral and dorsal rami; the ventral ramus passes across the back of the joint where it receives articular branches that form the LAAJ’s sensory supply; the dorsal ramus passes inferiorly and posteriorly, and its dorsal root ganglion lies behind the medial aspect of the lower part of the LAAJ.18 Another important anatomic relation of the LAAJ is the vertebral artery which lies immediately beside the joint’s lateral margin.
Biomechanics
Mobility of the spine is achieved primarily by the ways in which the ZJs move so as to make each pair of adjacent vertebrae a spinal motion segment. Every individual ZJ has the potential for the movements of translation (or gliding) and rotation in each of the three main anatomic planes—the sagittal, coronal (or frontal), and horizontal (or transverse) planes.19 Some of the six potential movements of each joint can only be achieved passively but all contribute to the mobility of the motion segment. The mobility of the spine as a whole is augmented by the ways in which the various spinal motion segments move in relation to each other giving the vertebral column ranges of extension and flexion in the sagittal plane, left and right side-bending in the coronal plane (also called lateral bending) and left and right rotation in the horizontal plane (also called axial rotation).
The shapes and orientations of the facets of the ZJs determine their contributions to stability and mobility. The typical cervical ZJs have surfaces that are more or less flat with a slight curvature so that from the side the upper facet looks slightly concave and the lower one slightly convex; the cervical joints are oriented at 90 degrees to the sagittal plane and at angles of about 45 degrees to both the coronal and horizontal planes so that the upper facet of each (that on the inferior articular process of the upper vertebra) faces forward and downward,19,20 as in Figure 36-2.
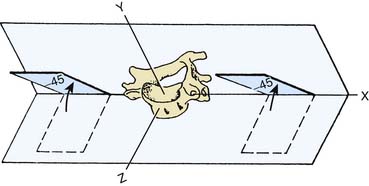
Figure 36-2 Orientation of the articular facets of a typical cervical zygapophysial joint.
(From White AA III, Panjabi MM: The basic kinematics of the human spine. A review of past and current knowledge. Spine 1978;3:12-20, with permission).
The facets of the thoracic ZJs are almost flat and oriented at an angle of about 20 degrees to the coronal plane. In this orientation, the upper facet of each faces forward,19,20 as in Figure 36-3.
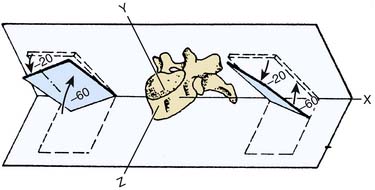
Figure 36-3 Orientation of the articular facets of a typical thoracic zygapophysial joint.
(From White AA III, Panjabi MM: The basic kinematics of the human spine. A review of past and current knowledge. Spine 1978;3:12-20, with permission).
The lumbar ZJs have correspondingly curved surfaces so that the upper facet of each is concave and the lower facet that matches it is convex. The lumbar joints are oriented mainly in the sagittal plane so that the concave upper facet faces laterally and slightly anteriorly, and the convex lower facet faces medially and slightly posteriorly,19,20 as in Figure 36-4.
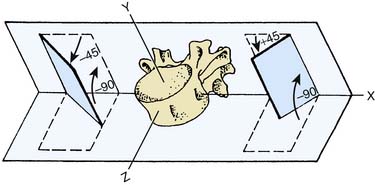
Figure 36-4 Orientation of the articular facets of a typical lumbar zygapophysial joint.
(From White AA III, Panjabi MM: The basic kinematics of the human spine. A review of past and current knowledge. Spine 1978;3:12-20, with permission.)
The cervical spine is the most mobile of the spinal regions because of its articular shapes and orientations, and the laxity of its joint capsules. The ranges of active movements of the cervical spine have been measured as up to 70 degrees each of extension and flexion (as determined by a radiographic study21), about 45 degrees of side-bending to each side and up to 40 degrees of rotation in either direction (as determined by a study using electric goniometers22). The ranges of side-bending and rotation are “coupled” so that they occur together, and to the same side, in the lower cervical spine (from C3 to C7; e.g., right side-bending is accompanied by right rotation). The passive ranges of cervical spinal movement have been measured as about 10 degrees more than the active ranges quoted in extension, flexion and side-bending to either side, and up to 50 degrees more in rotation to either side.23 Active and passive ranges of movement decrease as age increases.23
The movements of extension and flexion, side-bending, and rotation of each spinal motion segment occur around a central point known as the instantaneous axis of rotation (IAR).24 The position of the IAR in the segment determines the way the facets move in relation to each other as a ZJ goes through a range of movement. The positions of the IARs of cervical ZJ segmental motion have been determined—for example, the IAR of physiologic segmental extension in the cervical spine is located in the lower vertebral body of the segmental pair, near its upper end plate.24–,26
The thoracic spine is much less mobile and more stable than the cervical and lumbar spinal regions. The stability of the thoracic spine is enhanced by the coronal orientation of its ZJs, lesser degrees of laxity of their capsules, the supporting spinal ligaments, closer interlocking of the thoracic vertebrae, their long spinous processes, and the buttressing effect of the rib cage. The ranges of movement of the thoracic spine are difficult to measure experimentally in living subjects because the overlying ribs inhibit dynamic radiographic studies. A post mortem study of 10 specimens yielded an average range of about 60 degrees in the sagittal plane (i.e., of extension and flexion combined).27 The ranges are hard to discern clinically and in clinical practice the ranges of movement of the thoracic spine are usually assessed in conjunction with those of the lumbar spine.28
The ranges of active movements of the lumbar spine have been measured as up to 15 degrees of extension and 50° of flexion (as determined by several radiographic studies29–31), about 20° of side-bending to each side and up to 10 degrees of rotation in either direction.31,32 The movements of side-bending and rotation are coupled so that they occur together, and to opposite sides, in the upper lumbar spine (from L1 to L4); e.g., left side-bending is accompanied by right rotation in those motion segments.32 Side-bending and rotation occur to the same side in the L5-S1 segment and either way at L4-5 in different individuals.32 Extension and flexion also tend to be coupled with side-bending and rotation in the lumbar spine, but to varying extents in different subjects so that the coupling is much less predictable.32 As in the other spinal regions, the active ranges of lumbar movement decrease with increasing age.33,34
In the lumbar spine, as elsewhere, the movements of extension and flexion, side-bending, and rotation of the spinal motion segments each occur around an instantaneous axis of rotation (IAR). The positions of the IARs in the lumbar spine have been determined so, for example, the IAR of physiologic extension and flexion of a typical lumbar motion segment is located on the upper end plate of the lower vertebra of the segmental pair.35
The lumbar spine is stabilized by the mainly sagittal orientation of its ZJs (which limits side-bending and rotation), relatively taut ZJ capsules (compared to those of the cervical region), the anterior longitudinal ligament (which limits extension), the posterior longitudinal ligament, ligamentum flavum, and interspinous ligaments (which all limit flexion) the intertransverse and iliolumbar ligaments (which limit side-bending), and by the spinous processes (which limit extension). The resultant stability of the lumbar spine enables it to support the weight of the upper body in various postures at rest and during movements.
Static loading of the cervical spine is caused by the weight of the head and the tensions in cervical ligaments and muscles. The static load varies with posture; for example, it is low in lying with the head and neck supported, higher in upright sitting with the head and neck in the anatomic (neutral) position, and higher still with the head and neck at the end-ranges of extension and flexion.36
Static loading of the thoracic and lumbar spines results from the weight of the upper body, the tensions in thoracic and lumbar ligaments and muscles, and the effect of any additional load such as an object held in the hand. As in other spinal regions, static loading varies with posture. Lumbar static loading is relatively very low in supported supine lying, quite low in relaxed upright standing, higher in relaxed upright sitting, and progressively higher in standing with lumbar flexion and sitting with lumbar flexion.37
Dynamic loading of the thoracic and lumbar spines is a combination of static loading and any additional force(s) caused by active bodily movement or by the passive effects of loads applied with movement from external sources. For example, during ordinary walking, the dynamic loading of the lumbar spine varies with the phases of the gait cycle and is greatest at toe-off.38 In lifting an object while standing, dynamic loading of the lumbar spine is greater if the lumbar spine is flexed than if the back is kept straight, because the flexed position involves additional moments of force related to the distances of the upper body and the lifted object from the center of gravity.39,40
Zygapophysial Joint Pain
Mechanisms
Pain is defined “as an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”.41 The unpleasant emotional experience is mediated by unpleasant sensation, which begins with stimulation of sensory fibers of the peripheral nervous system. Peripheral sensory nerves have Ad and c nerve fibers that are sensitive to pain. Ad and c fibers are polymodal: they are sensitive to touch, vibration, proprioception, and thermal change as well as pain. In their role as pain sensors they are called nociceptors and the neurologic process of encoding and processing noxious stimuli which evoke pain is called nociception.42,43
ZJs have afferent sensory innervation including Ad and c fibers and so are capable of generating pain.5,15 Both the synovium and the capsule of each ZJ are richly supplied with nociceptor terminals. When they are stimulated in certain ways, pain will be generated from that joint. Pain generation was demonstrated in a study of normal volunteers; when ZJs were distended by injections of contrast medium, pain was evoked in patterns of distribution that were found to be reliable, recognizable, and joint-specific.12
Etiology
The unpleasant experience of pain begins with sensation that the brain interprets as actual or potential tissue damage.41 ZJ pain is initiated by mechanical loading of the tissues of one or more ZJ(s) at levels close to, or beyond, their load-bearing capacity. In such circumstances, the joint tissues are strained as the load is applied and if the load exceeds their capacity to resist, they will fail. In both phases of strain and then failure, nociceptors are stimulated, evoking pain.
The damaging forces that occur in motor vehicle accidents have been studied most. A cineradiographic in vivo study of cervical ZJs under loading in a simulated rear-end collision44 showed that under accident conditions the instantaneous axis of rotation moved upward and forward from its normal position in the lower vertebral body of a spinal motion segment to a position in the upper vertebral body of the pair. Movement around this “crash IAR” caused the ZJ facets to clash in unusual ways—often so that the posterior edge of the upper facet gouged into the surface of the lower facet. Other phenomena observed included the upper facet making impact on the anterior edge of the lower facet with shearing and compressive forces on both, and the facets gliding to different extents causing rupture of the joint restraints.
Another study using human cadaver head-neck complexes subjected to simulated motor accident conditions45 produced similar findings. The effects observed were consistent with what has been found in studies of the pathology of ZJ injuries, as set out in the next section.
Pathology
Several pathoanatomic studies have been undertaken to investigate the consequences of spinal structures being subjected to excessive forces.46–54 These studies have been based on post mortem examinations, some from autopsies conducted on individuals who had died in circumstances likely to have injured their spines, and some from autopsies conducted on those who died in other circumstances but were known to have had spinal pain from injuries sustained previously, some many years before death. Most of the studies also included radiologic examination of the spine to investigate any relationship between pathoanatomic findings and radiographic appearances.
In the cervical spine, these studies showed that injuries of the cervical ZJs and interbody joints are common consequences of spinal trauma but many of the injuries found involved only the soft tissues of the joints and were undetected by plain radiography.48,50–53 In one study of 22 spines, 19 (86%) were found to have ZJ injuries, many of which were at multiple levels. Sixty-nine injured ZJs were observed; of these only three subjects (14% of the study population) were found by radiography to have ZJ injuries, and in each case, only one ZJ injury was detected radiographically. So of the 69 injuries observed at autopsy, 66 (96%) went undetected by radiographic studies.50 In another study of 45 spines from people who died in motor vehicle accidents, the investigators found soft tissue injuries of the cervical ZJs in 72% of the sample but identified fractures in only 28% of them.51 The results of the other studies were similar. Studies of the cervical spines of those known to have suffered chronic neck pain and to have died in circumstances requiring autopsy (but unrelated to neck trauma) showed lesions in the cervical ZJs consistent with the long-term effects of the types of injuries observed in acute cases.51
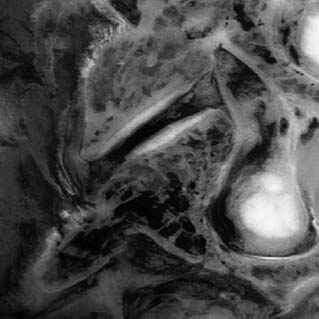
The cervical ZJ pathology observed in these studies was predominantly of soft tissues, which explains why most lesions were not detected by radiographic imaging. A range of pathologic lesions was found, including tears, splits, and partial loss of articular cartilage. In some cases, the full thickness of the articular cartilage was gouged away and this was often associated with injury of the surface layers of the subchondral bone (termed infraction), a lesion obvious on direct visualization or by special staining on microscopic preparations but not of such depth as to deform the bony surface grossly, so not detected radiographically. An example of full-thickness cartilage loss and infraction is shown in Figure 36-5. Other lesions observed included tearing of ZJ capsules and small undisplaced fractures of facet tips or of articular processes which did not appear on radiographs. In the chronic cases, the spines of those who had suffered spinal pain and died later of some other cause, pathologic changes observed included distortion of the joint surfaces with thinning of the articular cartilage and disruption of the articular cartilage.51,53
In the atlantooccipital and LAAJs, the pathologic lesions found were again mainly of articular soft tissues, the articular cartilages, and joint capsules. Also observed in conjunction with some soft tissue injuries at these levels were undisplaced fractures of the anterior and/or posterior arches of the atlas, of the odontoid process (or dens), and/or the arches of the axis.51,54
Pathoanatomic autopsy studies of the lumbar spine show that injuries of the lumbar ZJs are common consequences of spinal trauma as well. Again many of the injuries observed on dissection involve only the soft tissues of the joints and are undetected by plain radiography. In one study of 31 lumbar spines of individuals killed in motor vehicle accidents or other traumatic circumstances, 24 (77%) were found to have ZJ injuries, many of which involved more than one ZJ. Healed injuries of similar types were found in the spines of others who died of other causes but had been known to have a history of lumbar spinal pain since previous accidents. As in the studies of cervical injuries,48,50–54 few of the acute or chronic lumbar injuries were detected by plain radiography.47 Other studies have shown such injuries are not detected reliably by more sophisticated imaging modalities either (see later, in the section “Diagnosis of Zygapophysial Joint Pain”).
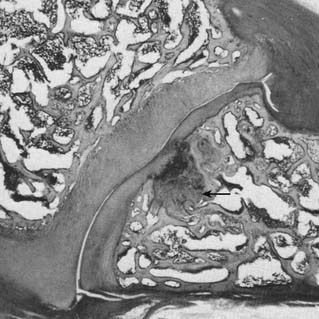
The lumbar ZJ pathology observed in the autopsy studies was also predominantly of soft tissues, which again explains why lesions were not detected by radiologic examination. The pathologic lesions found in lumbar ZJs were similar to those described in the cervical region: tears, splits, and gouging away of articular cartilage, infraction of subchondral bone (Fig. 36-6), tearing of joint capsules, and small undisplaced fractures of facet tips or of articular processes that did not show radiologically. In the spines of those who died after suffering lumbar spinal pain for a long time, pathologic changes observed in the ZJs included thinning of the articular cartilage, irregularity of the joint surfaces, and disruption of the joint capsule.47,49,51
Epidemiology
ZJ pain is common. It is one of the more common causes of spinal pain related to the neck, upper back, or lower back, and must be considered as a diagnostic possibility whenever a patient presents with any such symptom.55
The 12-month prevalences of chronic neck pain in the general adult population have been assessed as 1.7% (for more intense chronic neck pain that limits ability to work), 2.4% (for chronic neck pain that limits social activities), and 11.5% (for chronic neck pain that limits some activity).56 Studies show the prevalence of cervical ZJ pain among patients with chronic neck pain after motor vehicle accidents or similar trauma is at least 50%55–59 and in some circumstances may be as high as 80%.60 In those with lower neck pain the C5-6 level is most commonly affected and C6-7 is the next most commonly affected.58 Among patients whose dominant symptom after a motor vehicle accident is headache, the prevalence of pain stemming from the C2-3 ZJ has been assessed as between 37% and 68% with a mean of 53%.61,62
Chronic upper back pain related to the thoracic spinal region has been estimated to have annual prevalences in adult populations of between 5% and 10%.63,64 The prevalence of chronic thoracic ZJ pain among those with thoracic spinal pain has been determined as 48%.64
Chronic low back pain is very common in all countries. The point prevalence of chronic low back pain in general adult populations has been estimated as about 10% in Western countries such as Australia,65 New Zealand,66 the United Kingdom,67,68 and the United States69 and as high as 34% in the rural population of Tibet.70 The annual prevalence has been reported as between 13% and 49% in Western countries,71 42% in the rural population of Tibet,70 60% among Finnish reindeer herders,72 and from 60% to 83% among rural workers in China.73 The prevalence of lumbar ZJ pain has been determined as 30% to 40% among adults with chronic back pain in the United States.55,74 Age-related prevalences of lumbar ZJ pain have been measured in Australia, in studies based on definitive diagnosis by criterion standard methods, as 15% of younger adults with a history of injury and attending a pain clinic75 and 40% of older adults attending a rheumatology clinic.76 Both these studies showed the L5-S1 level is most commonly affected in the lumbar region, and the L4-5 level is the next most commonly affected.
Diagnosis of Zygapophysial Joint Pain
Clinical assessment, taking the medical history and performing a physical examination, may help the clinician to form an impression of the likely cause of a patient’s pain and should be carried out carefully and systematically in every case.77,78 However, there are no clinical features that are pathognomonic of ZJ pain at any spinal level, so the decision to test for ZJ pain cannot be validated on clinical grounds alone.
Some impression can be gained of the likelihood of a ZJ being the source of a patient’s pain by an informed consideration of the symptoms, and especially of the pain distribution and pain quality.77 The distribution of pain generated from a particular structure is called a “pain map.” Studies based on joint provocation in normal subjects and anesthetization of specific joints in those with chronic pain have resulted in pain maps being plotted for ZJs at all cervical,12,79–81 thoracic,82 and lumbar4,83–85 levels, and for the atlantooccipital and LAAJs.86,87 The quality of pain provides another useful clue. ZJ pain is typically dull and aching in quality, of the type called somatic pain (in a local distribution near the source) and somatic referred pain when it is perceived in more distant regions.88,89 Other spinal structures may also generate somatic pain, so it is not specific to ZJs, but it is quite different from radicular pain, the sharp, shooting, and sometimes “electric” pain associated with nerve root irritation.90
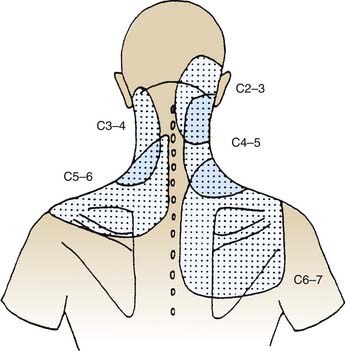
The pain maps of cervical ZJs are depicted in Figure 36-7. If a patient presents with somatic and/or somatic referred pain in the neck, in the lower neck and shoulder, or in the upper neck and head (so-called cervicogenic headache91,92) in a distribution like one of those described in Figure 36-7, it may be suspected to be of cervical ZJ origin. The pain maps provide clues to the level of a joint that may be a pain source but do not identify a level specifically because the maps overlap considerably: each part of a patient’s neck lies in at least two, and perhaps as many as four, of the areas to which pain may be referred from particular joints.
When a patient presents with what is suspected to be cervicogenic headache, the lateral atlantoaxial (C1-2) and atlanto-occipital (C0-1) joints must also be considered as possible sources. The pain maps of those joints are depicted in Figures 36-8 and 36-9. The pain maps of the C0-1, C1-2, C2-3, and C3-4 joints also overlap considerably, so although they provide clues to the possible origin of cervicogenic headache, they do not, in themselves, enable identification of the source. In the thoracic spinal region the pain maps overlap as well. The distribution of pain from a thoracic ZJ is to an adjacent zone of the upper back, lateral to the joint and from half a spinal segment higher to a full segment lower as shown in Figure 36-10.
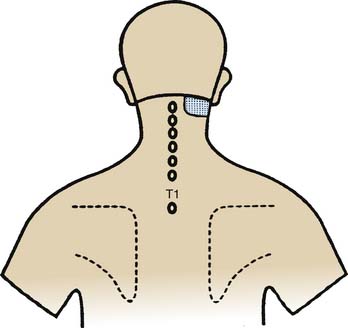
Figure 36-8 Pain map showing the pattern of distribution of lateral atlantoaxial (C1-2) joint pain.
(From Dreyfuss P, Michaelsen M, Fletcher D: Atlanto-occipital and lateral atlanto-axial joint pain patterns. Spine 1994;19:1125-1131, with permission.)
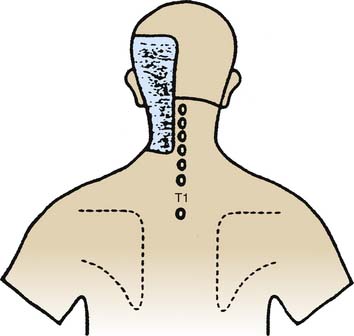
Figure 36-9 Pain map showing the pattern of distribution of atlantooccipital (C0-1) joint pain.
(From Dreyfuss P, Michaelsen M, Fletcher D: Atlanto-occipital and lateral atlanto-axial joint pain patterns. Spine 1994;19:1125-1131, with permission.)
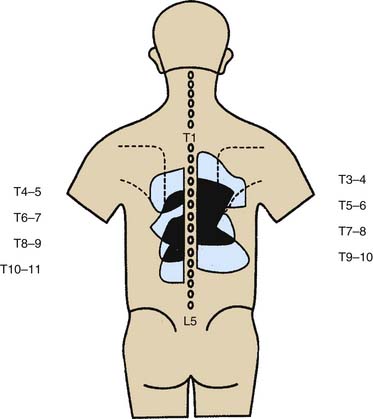
Figure 36-10 Pain maps showing patterns of distribution of thoracic zygapophysial joint pain.
(From Dreyfuss P, Tibiletti C, Dreyer SJ: Thoracic zygapophyseal joint pain patterns. A study in normal volunteers. Spine 1994;19:807-811, with permission.)
Lumbar ZJ pain maps are comparable. Somatic pain from a lumbar ZJ occurs in an adjacent zone of the lower back, lateral to the joint, and from about one spinal segment higher to one segment lower, with somatic referred pain extending down the back of the leg. The patterns overlap to a considerable extent with each joint generating pain to a slightly lower level than that of the joint above it. The overlap makes it difficult to depict individual maps in a single diagram but the composite pattern of distribution is as shown in Figure 36-11.
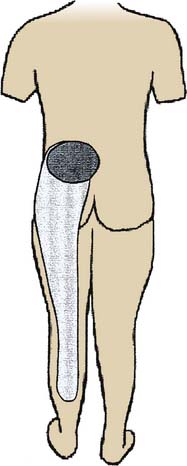
Figure 36-11 Pain map showing patterns of distribution of somatic and somatic referred pain of lumbar zygapophysial joint origin.
(From Bogduk N, McGuirk B: Medical management of acute and chronic low back pain: an evidence-based approach. Amsterdam, Elsevier, p 9, 2002, with permission.)
Physical examination is a traditional component of clinical assessment and it is valuable for helping the clinician develop an impression of the patient and the problem. However, clinical examination findings provide few clues to the likelihood of pain being of ZJ origin and there is no physical sign, or combination of signs, that enables identification of a particular ZJ as a source of pain. By convention, physical examination of the musculoskeletal system includes inspection, palpation, and testing of movements (which includes assessing active, passive, and accessory ranges of movement, and challenging the restraints to movement).78 If the clinician examines the patient systematically and addresses all these domains, many signs will be elicited but care must be exercised in interpreting them in the light of the scientific evidence of their reliability and validity.
Data on the reliability of inspection of the various regions of the spine for lordosis, kyphosis, and scoliosis show interobserver agreement to be low, with Kappa scores from 0.13 to 0.39.93,94 Data on the reliability of palpation of the spine for tenderness at specific sites also show interobserver agreement to be low, with Kappa scores from 0.11 to 0.53.95–97 The reliability of assessing gross ranges of active spinal movement seems somewhat better, in some ranges at least, with, for example, reported Kappa scores of 0.40 for cervical rotation and 0.56 for cervical extension,95 from 0.35 to 0.74 for lumbar extension,94 but only from 0.11 to 0.43 for lumbar side-bending.94 The reliability of testing passive intervertebral movements is very poor, with Kappa scores in negative ranges.93,98
Reliability is one thing but reliability data only show the consistency of observations, not what those observations can be interpreted to mean. Such interpretation must be based on evidence of validity. There is very little evidence of the validity of physical examination in the diagnosis of ZJ pain. There are no sound data on the validity of inspection or testing gross ranges of movement in the diagnosis of ZJ pain in the cervical, thoracic, or lumbar regions. There are no sound data on the validity of palpation in the diagnosis of thoracic or lumbar ZJ pain. Such data as exist on the validity of physical examination relate to palpation for specific physical signs in the assessment of patients with neck pain. There are data99 showing certain physical tests are valid, with positive likelihood ratios of from 2.7 to 12.8, for confirming that pain is of spinal origin but not for identifying the specific source of that pain.
The data from two validity studies show that manual examination is not valid for diagnosis of cervical ZJ pain. A small set of data from a preliminary study100 seemed to show that manual examination was valid for the identification of a painful cervical ZJ and much faith was placed on that evidence by manual therapists for some time thereafter. However, the data set was small and the authors of that early study called for further research to be done before their results were generalized. In response to that call, a larger study101 was done and its results showed clearly that manual examination is not valid for the diagnosis of cervical ZJ joint pain; the positive likelihood ratios were only from 1.4 to 1.8. Reassessment of the data of the earlier study, in the light of later knowledge of aspects such as the rate of false-positive results, showed the results of both studies are consistent and both actually show manual examination is invalid for the purpose. The summary of the evidence on clinical assessment is that some guidance is provided by established patterns of distribution of pain from individual joints, the so-called spinal pain maps, but there are no clinical methods that are valid for identifying specific painful ZJs.
Imaging studies provide information about the spine and traditionally imaging has been used in the assessment of patients with spinal pain, but imaging results do not identify painful spinal joints. The imaging modalities used most often are plain radiographs, computer assisted tomographic (CAT or CT) scanning, magnetic resonance imaging (MRI), and isotopic bone scans. These frequently show radiologic appearances of spondylosis or osteoarthrosis, including joint space irregularity and narrowing, subchondral bony sclerosis, subchondral cysts, periarticular bony hypertrophy, and the presence of osteophytes. These changes, sometimes incorrectly called “degenerative changes,” reflect the normal responses of the articular cartilage and the subchondral bone to the repeated biomechanical stresses of daily living.102,103 It is often assumed that there is a causal relationship between these imaging changes and pain generation but the scientific evidence suggests otherwise. The fact that the changes are age-related is clearly demonstrated by the results of numerous studies showing direct correlation between their prevalence and increasing age.104–109 The fact that they are not regularly associated with pain is borne out by the results of numerous studies showing no correlation between the presence of pain and spondylotic changes shown by plain radiography,110–116 CT scanning,117 and MRI.118–121
No other radiologic appearances seen on plain radiography,122,123 CT scanning,124 MRI,125,126 or any other imaging modality have been proved to be correlated with ZJ pain. Thus, after comprehensive clinical assessment and imaging, the clinician may gain the impression that a patient’s pain may be of ZJ origin, but that impression cannot be confirmed by clinical features and/or imaging results—separately or in combination.
The only way of determining that a ZJ is (or is not) a source of pain is to test it by anesthetic blockade of that joint alone, to see if the pain is abolished by the blockade: such tests are called diagnostic joint blocks. If a decision to undertake ZJ blocks is made, the next issue is which joint to test first. That decision will depend on the clinical impression; further guidance may be obtained from the prevalence data set out earlier under “Epidemiology”. As stated there, in the cervical spine, the ZJs most often involved in cervicogenic headache are those at the C2-3 level58 and the joints most often associated with lower neck pain are those at C5-6.62 There are no prevalence data for specific segmental origins of thoracic ZJ pain. In the lumbar spine, the ZJs most often involved in pain generation are those at the L5-S1 level.75
Indications for Interventions
When contemplating specific indications for interventions in the management of ZJ pain, the first consideration is the duration of the condition. By convention, conditions are classified by their time courses as acute and chronic.127 Acute pain is defined as that of short duration which is likely to settle spontaneously by natural healing of the causative condition. Chronic pain is defined as that which persists beyond the normal time of natural healing.128,129 After much discussion among clinicians and researchers about how long should be allowed for natural healing, acute pain was defined as pain present for up to 3 months and chronic pain was defined as pain present for more than 3 months.130
Acute spinal pain, in most cases, will resolve by natural healing if just left alone.131–133 Clinicians who do not appreciate this phenomenon often use interventions to treat acute spinal pain when to do so is unlikely to shorten the course of the condition and may even lengthen it. Active interventions are actually contraindicated for most acute spinal pain. What patients with acute spinal pain need is explanation of the favorable natural history, reassurance, pain relief (by analgesic medication or some other method) and encouragement to remain active; beyond that all they need is follow-up until the pain settles.131–133
Chronic spinal pain usually persists until effective treatment is applied, so intervention is indicated in virtually every case. Some clinicians seem unaware of the evidence in this regard and manage chronic spinal pain as if its cause is unidentifiable and only general measures can be applied to help the patient live with the problem. That approach is outmoded. These days the causes of most chronic spinal pain can be identified precisely and many of those identifiable causes can be treated effectively. That is certainly the case for chronic ZJ pain. The key to the management of chronic spinal pain is precise diagnosis.134
The specific indications for a diagnostic intervention in the management of chronic ZJ pain are (1) the patient is likely on the basis of their clinical presentation to have chronic ZJ pain, (2) the intervention planned is known to be useful for determining whether ZJ pain is present or not, and if so from which joint(s), and (3) the intervention is justified in terms of its safety, therapeutic utility, personal utility for the patient and cost-effectiveness, and the patient has given informed consent.
Medial Branch Blocks
Development
Medial branch blocks are local anesthetic blocks of the articular nerves (the medial branches) that transmit sensory information including nociceptive signals from ZJs (as described earlier under “Mechanisms”). Historically, the first method used to test a ZJ as a possible source of pain was injection of local anesthetic into the cavity of a lumbar ZJ84; such tests are called intraarticular blocks (IABs). Comparable techniques were developed for cervical135 and thoracic136 ZJs as well. Later, less invasive methods were developed to achieve blockade of a specific joint by blocking the articular nerve(s) outside the joint137,138; such tests are designated by the particular nerves involved as medial branch blocks (MBBs) and third occipital nerve blocks (TONBs). Because articular nerve blocks are less invasive and are performed more often to investigate the common sources of chronic spinal pain, they will be described first.
Cervical Medial Branch Blocks C3 to C6—Procedure
A cervical medial branch block procedure involves a lot more than the needling and injection commonly associated with the name. This is also true for other such procedures. Each diagnostic procedure involves three phases, a preoperative phase, an operative needling phase, and a postoperative observational phase. The full test process involves a fourth phase, the interpretation of individual block results and the integration of the information they provide in the overall process of diagnosis. If a medial branch block is thought of mainly as the needling part, the other phases may be given less emphasis than they deserve and the whole process may be compromised.
Each cervical ZJ from C3-4 down to C6-7 is supplied by two medial branches, the medial branches of the cervical dorsal rami above and below the joint. Thus, the C5-6 ZJ is supplied by the C5 medial branch and the C6 medial branch. The procedure to test the C5-6 ZJ as a pain source involves blocking each of those two nerves. The courses of the medial branches have been plotted by cadaveric dissection studies and shown to lie more or less horizontally across the middle parts of the articular pillars that join the superior and inferior articular processes of each vertebra.139 The courses of these medial branches are illustrated in Figure 36-12.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


