TOPICS
1. Intra-aortic balloon counterpulsation and the heart surgery patient
2. Ventricular assist devices: designs and indications
5. Anesthetic management of VADs
Adult heart surgery patients are increasingly older with varying degrees of preoperative ventricular failure. Patients routinely present with both systolic and diastolic ventricular dysfunction, ventricular remodeling, fluid retention, and pulmonary congestion. Additionally, even those patients with well-preserved ventricular function preoperatively can deteriorate intraoperatively secondary to inadequate myocardial preservation, embolism, myocardial ischemia, protamine reactions, and other “catastrophic” events (eg, anaphylaxis, aortic dissection, etc). Of course, the overwhelming majority of patients experiencing intra-operative right or left ventricular failure can be treated with a combination of inotropes and nitric oxide inhalation. However, others lack sufficient ventricular function to provide adequate delivery of oxygenated blood to the tissues. Such patients readily develop renal dysfunction, acidosis, and ultimately die from cardiogenic shock unless provided mechanical assistance to support or replace the heart’s pump function. This chapter reviews the anesthetic management of patients in need of intra-aortic balloon counterpulsation, (IABP) ventricular assist devices (VADs), and heart transplantation (HT).
INTRA-AORTIC BALLOON COUNTERPULSATION AND THE HEART SURGERY PATIENT
IABP counterpulsation is employed to assist the failing heart (Video 11–1). It is not a substitute for a beating ventricle and as such does not replace the function of the ventricle it is assisting. The patient must have some cardiac output even if not adequate. IABP is generally introduced via the femoral artery into the thoracic aorta and positioned distal to the take off of the left subclavian artery. The IABP inflates with carbon dioxide or helium during diastole and deflates during systole. Thus, it creates a counterpulsation to the pulsation generated by the heart. By inflating during diastole at the point of aortic valve closure, they augment diastolic blood pressure and thus improve coronary perfusion pressure (CPP) of the left ventricle (LV).
Recall,
CPP = Diastolic blood pressure (DBP) − Left ventricular end diastolic pressure (LVEDP)
During systole, the IABP deflates reducing the afterload against which the heart must eject, thereby potentially improving forward blood flow.
The cardiac anesthesiologist is likely to encounter the IABP in several situations:
1. Many patients presenting with myocardial ischemia refractory to medical or percutaneous interventions are provided an IABP in the cardiac catheterization laboratory to relieve ischemic chest pain. By increasing DBP and lowering LVEDP, the IABP can improve the balance of LV myocardial oxygen supply and demand. In a 1997 review of 4756 IAPB uses in a single institution over a period of 30 years, Torchiana et al suggested that preoperative placement of an IABP in those with medically refractory ischemia can improve patient outcome.1
2. In patients with cardiogenic shock, the IABP is placed to augment cardiac output in the immediate preoperative period should emergent heart surgery be warranted. Of note, the IABP is contraindicated in patients with aortic dissections, aortic aneurysms, severe aortic insufficiency, and severe atherosclerotic disease in the descending aorta.
3. IABPs are placed in the operating room in those patients whose poor ventricular function prohibits separation from cardiopulmonary bypass (CPB) in spite of maximal inotropic and vasopressor support.
4. In patients with a sudden-onset ventricular septal defect (VSD) or papillary muscle/chordal rupture secondary to acute myocardial infarction, the IABP is placed to reduce afterload, hence decrease left-to-right shunt or MR respectively.
Several parameters are important for the adequate operation of the IABP and can be set up from the IABP console. Synchronization of the IABP with the native cardiac rhythm and timing of the balloon inflation and deflation can be done using either the ECG tracing or the arterial pressure tracing. The arterial pressure rise during balloon inflation occurs with the dicrotic notch of the arterial waveform, which signifies the closure of the aortic valve and the beginning of diastole. Timing of the inflation and deflation of the IABP is critical to achieve maximal diastolic augmentation of the blood pressure and maximal afterload reduction. Another parameter that can be set up is the ratio of IABP pulsations to native ventricular pulsations. The IABP can cycle with every beat (1 to 1 assist), every other beat, or every fourth beat of the heart. In this way the degree of assist can be regulated when the patient is to be weaned from IABP support. The volume of gas used to inflate the balloon and the time required for inflation and deflation can also be setup.
Complications of IABP use include femoral artery injuries, arterial dissections, thromboembolism, and balloon rupture with gas embolism and some of these complications require exploration of the femoral artery and arterial embolectomy.
VENTRICULAR ASSIST DEVICES: DESIGNS AND INDICATIONS
Unlike IABPs that require a working left ventricle producing some cardiac output to be effective, ventricular assist devices (VADs) can function in place of a completely dysfunctional left or right ventricle. VADs are often placed when medical therapy has been exhausted to improve cardiac function. Since deteriorations in ventricular failure can occur both acutely and chronically, VAD placement can be either elective or emergent.
The decision to place a VAD and the type of device to be employed is dependent upon both the patient’s associated illnesses and the estimated time that VAD therapy will be required. VADs can be placed to provide short-term ventricular support in those cases where recovery of cardiac function or heart transplantation (HT) is expected. Both percutaneous and implantable devices have been used in this setting. At other times, recovery of the heart function is not considered likely and VADs are placed to support organ perfusion in patients awaiting heart transplantation. Still, other patients are thought not to be suitable candidates for the limited number of hearts available for transplantation and are provided a VAD as so-called “destination” therapy. In other words, it is hoped that the VAD will improve ventricular function sufficiently to provide these patients crippled by heart failure both longer and better quality lives. The decision to commit an individual to VAD support is not lightly undertaken and should be considered in situations when kidney, liver, pulmonary, and neurologic dysfunction are not so advanced that patient survival is not thought possible even with improved cardiac output. Usually, the patient’s cardiologist together with a cardiothoracic surgeon will determine whether VAD as “destination” therapy or HT is warranted. Although anesthesiologists are heavily involved in the perioperative placement of these devices, they generally will not be a part of the discussion with the patient and their family regarding the decision to place the device. However, emergent VAD placement in the setting of failure to separate from cardiopulmonary bypass (CPB) should occur only after the surgeon and the anesthesiologist discuss the immediate patient management plan.
VADs are used to support the function of the left, right, or both ventricles. They can be classified according to how blood flows when they are employed. Flow through a VAD can be either continuous or pulsatile. Continuous flow VADs include devices placed percutaneously for temporary support of ventricular function (eg, Impella) and devices implanted (eg, HeartMate II). Pulsatile VADs include extracorporeal devices (eg, Abiomed BVS) for short-term support and those for support of longer duration (eg, HeartMate I).2
SHORT-TERM VAD PLACEMENT
VADs can be placed emergently whenever ventricular function is severely compromised. Often candidates for emergent VAD placement are in cardiogenic shock requiring multiple vasoactive medications and possible IABP counterpulsation. VAD placement may prevent the development of multiorgan system failure giving time for the heart to recover function or may provide a “bridge to decision” during which the patient, his healthcare providers, and family members can discern the best course of therapy.
The type of VAD to be placed and whether one or both of the ventricles will be supported depends upon the clinical conditions. A left ventricular assist device (LVAD) is placed in the setting of cardiogenic shock and poor left ventricular systolic function (Video 11–2A and 11–2B). A right ventricular assist device (RVAD) is placed when the right heart fails such as during a right ventricular infarction or in patients with severe pulmonary artery hypertension. In this setting the LV is often underloaded as the RV does not deliver sufficient blood to the LV to eject into the systemic circulation resulting in cardiogenic shock. At times, both ventricles require mechanical support. However, LVAD placement will sometimes sufficiently unload the left ventricle such that flow through the RV improves eliminating the need for biventricular VAD (BIVAD) placement.
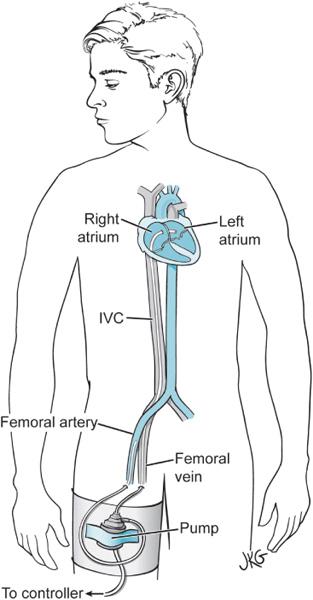
Emergent short-term VADs include both percutaneously and surgically placed devices. Percutaneous devices can be placed in the cardiac catheterization laboratory and thus can provide mechanical assistance without the need for surgical interventions. The TandemHeart3–5 device provides left atrial-to-femoral artery blood flow. TandemHeart is a continuous flow centrifugal device using an extracorporeal pump. The inflow cannula is inserted via the femoral vein through the intra-atrial septum into the left atrium. Oxygenated blood is then pumped from the left atrium and returned to the systemic circulation via a cannula placed in a femoral artery providing retrograde flow to most of the body. Since the lungs continue to oxygenate blood flowing into the left atrium, TandemHeart can be employed during high-risk percutaneous coronary interventions (PCIs) to provide circulatory support without requiring extra corporeal oxygenation (Figure 11–1). Although TandemHeart was capable of improving hemodynamics in a randomized trial of patients with cardiogenic shock following acute myocardial infarction compared to those treated with IABP support, the 30-day mortality was similar between the groups.4
The Impella Recover is another percutaneous device, which can be used to support left ventricular function.6 The device can be placed via the femoral artery or alternatively placed directly into the aorta intraoperatively and threaded across the aortic valve into the left ventricle. Patients with postoperative LV failure treated with an Impella Recover device were found to have a similar mortality to that of patients supported with an IABP.6 However, in the patients whose native hearts could produce 1 L/min of cardiac output the Impella device showed better long-term survival compared with an IABP. Both the Impella device and TandemHeart require anticoagulation.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


