
After thorough debridement, the skin from the amputated part is used for cover and closure creating a useful esthetic four-finger hand.

18.3 Case 2
Arm gunshot injury to ulnar nerve with gap of 8 cm.
The gap was bridged by nerve allograft.
18.4 Case 3
A child referred after initial treatment for a right forearm amputation and injury to the left hand with severe adduction contracture.


Right forearm got a useful prosthesis.

Left hand’s first web space opened by gradual elongation of external fixation between the first and second metacarpal bones.

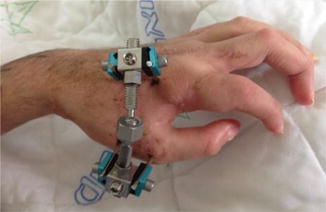
Good abduction was achieved with subluxation of the first carpometacarpal joint. The external fixation was replaced by plaster cast allowing spontaneous relocation of the joint.


Cast removal followed by intensive guided exercises.
18.5 Case 4
Comminuted displaced fracture of the medial condyle of the elbow by blast injury.

 Things Aren’t Always What They Seem: The Case of Hala
Things Aren’t Always What They Seem: The Case of Hala
 Pelvic Injury
Pelvic Injury
 Multiple Malformations Embryo in a Syrian Pregnant Patient
Mediastinal Masses
Multiple Malformations Embryo in a Syrian Pregnant Patient
Mediastinal Masses
 Nonconventional Management of Bleeding Dysgerminoma in Adolescent Syrian Female
Nonconventional Management of Bleeding Dysgerminoma in Adolescent Syrian Female
 Acute Shortening and Angulation for Limb Salvage in Pediatric Patient After High-Energy Blast Injury
Acute Shortening and Angulation for Limb Salvage in Pediatric Patient After High-Energy Blast Injury




Related posts:
Things Aren’t Always What They Seem: The Case of Hala
Pelvic Injury
Multiple Malformations Embryo in a Syrian Pregnant Patient
Mediastinal Masses
Nonconventional Management of Bleeding Dysgerminoma in Adolescent Syrian Female
Acute Shortening and Angulation for Limb Salvage in Pediatric Patient After High-Energy Blast Injury
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
