Ultrasound-Guided Proximal Parasacral Block
Kevin King
Jacques E. Chelly
 Background and indications: The parasacral block was originally described using a landmark approach and neurostimulation. Early reported success rates range from 60% to 90%. The use of ultrasound may enable the practitioner to improve on this success rate as well as to avoid some of the described complications and side effects associated with the performance of this block. The sacral plexus originates from roots L4, L5, S1, S2, and S3. The roots emerge from the deep surface of the sacrum, where they join to form the sciatic nerve and its tributaries. It leaves the pelvis at the level of the greater sciatic foramen. At this level, the nerves are covered by the gluteus maximus and the piriformis muscles. After the sciatic nerve passes underneath the piriformis muscle, it extends caudally and passes over the superior and inferior gemelli muscles and the obturator internus muscles (Fig. 28.1). The parasacral plexus block allows the anesthesiologist to block the sciatic nerve, the posterior femoral cuTaneous nerve, and the superior gluteal nerve, which contributes articular sensory branches to the posterior capsule of the hip.
Background and indications: The parasacral block was originally described using a landmark approach and neurostimulation. Early reported success rates range from 60% to 90%. The use of ultrasound may enable the practitioner to improve on this success rate as well as to avoid some of the described complications and side effects associated with the performance of this block. The sacral plexus originates from roots L4, L5, S1, S2, and S3. The roots emerge from the deep surface of the sacrum, where they join to form the sciatic nerve and its tributaries. It leaves the pelvis at the level of the greater sciatic foramen. At this level, the nerves are covered by the gluteus maximus and the piriformis muscles. After the sciatic nerve passes underneath the piriformis muscle, it extends caudally and passes over the superior and inferior gemelli muscles and the obturator internus muscles (Fig. 28.1). The parasacral plexus block allows the anesthesiologist to block the sciatic nerve, the posterior femoral cuTaneous nerve, and the superior gluteal nerve, which contributes articular sensory branches to the posterior capsule of the hip.The performance of the parasacral block is associated with a risk of bowel or rectum perforation, as the pelvic aponeurosis lies immediately deep to the parasacral plexus. This aponeurosis or fascia is often poorly visualized on ultrasound except in athletes and very thin individuals. It is impossible to appreciate in a blind technique. Parasacral block may also anesthetize the pudendal and other sacral nerves that lie nearby. Parasacral block can be used for surgical anesthesia of the hip or knee in conjunction with lumbar plexus block.
 Anatomy: Due to the depth of the sacral plexus, practitioners may wish to combine stimulation with ultrasound guidance. The probe is placed at 6 to 8 cm caudal to the posterior superior iliac spine (PSIS) along the line joining ischium and the PSIS (Fig. 28.2). Utilizing ultrasound, the landmarks include the PSIS and ischial tuberosity (IT) and the gluteus maximus and the piriformis muscle and gluteal artery (Figs. 28.2 28.3 and 28.4A to C). The sacral plexus is a flat hyperechoic structure at the same depth as the ischium and sacrum.
Anatomy: Due to the depth of the sacral plexus, practitioners may wish to combine stimulation with ultrasound guidance. The probe is placed at 6 to 8 cm caudal to the posterior superior iliac spine (PSIS) along the line joining ischium and the PSIS (Fig. 28.2). Utilizing ultrasound, the landmarks include the PSIS and ischial tuberosity (IT) and the gluteus maximus and the piriformis muscle and gluteal artery (Figs. 28.2 28.3 and 28.4A to C). The sacral plexus is a flat hyperechoic structure at the same depth as the ischium and sacrum. Patient position: Lateral decubitus with the operative side up. The hip and knee are flexed.
Patient position: Lateral decubitus with the operative side up. The hip and knee are flexed. Transducer: 60-mm curved array oscillating at 2 to 5 MHz.
Transducer: 60-mm curved array oscillating at 2 to 5 MHz. Transducer position: Transverse in horizontal plane over superior medial aspect of buttock.
Transducer position: Transverse in horizontal plane over superior medial aspect of buttock.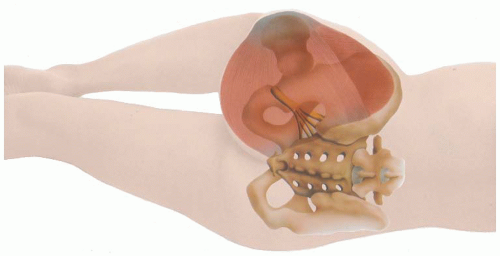 Figure 28.1. Illustration of the parasacral sciatic nerve roots. |
Related posts:
 Microanatomy of the Peripheral Nervous System and Stimulation Thresholds Inside and Outside the Epineurium
Microanatomy of the Peripheral Nervous System and Stimulation Thresholds Inside and Outside the Epineurium
 Ultrasound-Guided Intraneural Injection—The Human Data
Ultrasound-Guided Intraneural Injection—The Human Data
 Ultrasound-Guided Blocks at the Elbow and Forearm
Ultrasound-Guided Blocks at the Elbow and Forearm
 Ultrasound-Guided Anterior Sciatic Nerve Block
Ultrasound-Guided Anterior Sciatic Nerve Block
 Ultrasound-Guided Caudal, Lumbar, and Epidural Injection
Ultrasound-Guided Caudal, Lumbar, and Epidural Injection
 Ultrasound-Guided Genitofemoral Nerve Block
Ultrasound-Guided Genitofemoral Nerve Block
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


