Ultrasound-Guided Medial Paravertebral Block, Lateral Paravertebral Block, Pectoral Block, and Serratus Anterior Block
Part 1: Medial and Lateral Paravertebral Block
Paul E. Bigeleisen
Alon Ben-Ari
Andrea Fanelli
Daniela Elena Francesca Ghisi
 Background and indications: Thoracic paravertebral blocks have been shown to provide unilateral or bilateral anesthesia and postoperative analgesia comparable to thoracic epidural anesthesia and analgesia.1,2 In addition, paravertebral blocks have decreased the recurrence of cancer in a retrospective study.3
Background and indications: Thoracic paravertebral blocks have been shown to provide unilateral or bilateral anesthesia and postoperative analgesia comparable to thoracic epidural anesthesia and analgesia.1,2 In addition, paravertebral blocks have decreased the recurrence of cancer in a retrospective study.3Thoracic paravertebral blocks are performed by injecting the local anesthetic solution into the paravertebral space, which contains the thoracic nerves, their branches, and the sympathetic trunk. Thoracic paravertebral nerve blocks can be used for patients undergoing many types of surgery and also for those with trauma pain and chronic pain. The indications include anesthesia and postoperative analgesia for breast surgery, videoassisted thoracoscopies, ventral hernia repairs, and postoperative analgesia after major and minor thoracic and abdominal procedures.4 Compared to neuraxial blocks, paravertebral blocks can be managed in the presence of a moderate degree of hemostatic deficiency: a careful bAlance of risks and benefits rather than a dogmatic and rigid approach is suggested.5 Urinary retention and pruritus are not concerns. There is a small risk of pneumothorax. Occasionally, injections may enter the epidural space. The rate of absorption of local anesthetics by the pleura is high; thus, toxicity has been described as a possible side effect.
Several methods to reach the paravertebral space have been described. The classic technique for the paravertebral block uses a blind approach: The needle is inserted 2.5 to 4 cm lateral to the posterior spinous process in search of the transverse process. When the transverse process is contacted, the needle is withdrawn and redirected caudal to the transverse process, approximately 1 cm deeper than the transverse process.6, 7and 8 Once the costotransverse ligament is pierced, local anesthetic is injected.
A loss-of-resisTance technique was described by Eason and Wyatt.9 More recently, Richardson et al.10 introduced a pressure-measurement technique in which the correct needle tip position within the paravertebral space is detected by different pressure values. An autodetect syringe was used also by Mundey et al.11 for loss-of-resisTance technique. Recent advances in ultrasonography have made it possible to place the needle in the paravertebral space under direct ultrasound guidance.12,13
 Anatomy: The thoracic paravertebral space, in sagittal cross section, is triangular. Its boundaries include posteriorly the superior costotransverse ligament, the transverse processes, and the ribs above and below the intercostal nerve and vessels; medially, the boundary includes the rib and vertebral foramen. The endothoracic fascia forms the deep border of the space and separates the nerve roots from the sympathetic ganglia (Fig. 37.1A,B).
Anatomy: The thoracic paravertebral space, in sagittal cross section, is triangular. Its boundaries include posteriorly the superior costotransverse ligament, the transverse processes, and the ribs above and below the intercostal nerve and vessels; medially, the boundary includes the rib and vertebral foramen. The endothoracic fascia forms the deep border of the space and separates the nerve roots from the sympathetic ganglia (Fig. 37.1A,B).In most cases, the endothoracic fascia cannot be visualized on ultrasound, and the pleura, which lies immediately deep to the endothoracic fascia, is used as a landmark to prevent the
needle from being inserted too far. In thin patients, the epidural space, the transverse process, the costotransverse ligament, and the pleura can be imaged in sagittal view by placing the transducer lateral to the posterior spinous process and toggling from medial to lateral.
needle from being inserted too far. In thin patients, the epidural space, the transverse process, the costotransverse ligament, and the pleura can be imaged in sagittal view by placing the transducer lateral to the posterior spinous process and toggling from medial to lateral.
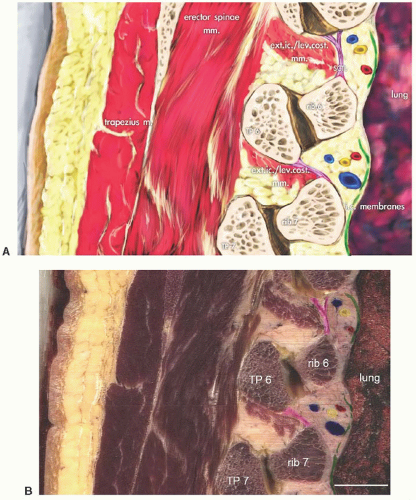 Figure 37.1. A: Drawing of the paravertebral space in sagittal section. ext.ic./lev. cost. mm., external intercostal/leverator costalis muscles; i.c., intercostal; m. and mm., muscle; SCTL, superior costotransverse ligament; TP6 and TP7, transverse process of sixth and seventh vertebral bodies. B: CadavEric image of the paravertebral space in sagittal section. TP6 and TP7, transverse process of sixth and seventh vertebral bodies. |
 Transducer: A 4- to 6-cm linear probe oscillating at 8 to 12 MHz may be used in small patients. If the pleura is located deeper than 4 cm, a 4- to 6-cm curved probe oscillating at 2 to 5 MHz is recommended.
Transducer: A 4- to 6-cm linear probe oscillating at 8 to 12 MHz may be used in small patients. If the pleura is located deeper than 4 cm, a 4- to 6-cm curved probe oscillating at 2 to 5 MHz is recommended. Needle
NeedleSingle-Shot Thoracic Paravertebral Block: 21G, 9-cm, Tuohy needle.
Continuous Thoracic Paravertebral Block: 18G, 9-cm, Tuohy needle.
 Local anesthetic: Single-injection thoracic paravertebral blocks.
Local anesthetic: Single-injection thoracic paravertebral blocks. Anesthesia: Mepivacaine 1.5%, 3 to 5 mL for each level.
Anesthesia: Mepivacaine 1.5%, 3 to 5 mL for each level.If postoperative analgesia is required: ropivacaine 0.5% or levobupivacaine 0.375% to 0.5%, 3 to 5 mL for each level or 15 mL injected at a single level.
Continuous thoracic paravertebral blocks
Continuous infusion: ropivacaine 0.2% or levobupivacaine 0.125%, 5 to 10 mL/h.
Programmed intermittent anesthetic bolus: ropivacaine 0.2% or levobupivacaine 0.125%, 8 to 10 mL every 60 minutes.
 Techniques
TechniquesSagittal Approach: The patient is placed in a sitting position. The relevant thoracic spinous processes are palpated starting from C7 and marked on the skin (Fig. 37.2). A point 2.5 to 3 cm lateral to the tip of the spinous process is marked (Fig. 37.2). The region is scanned using a 2- to 5-MHz curved array transducer placed parallel to the spinous processes (sagittal) in search of the transverse processes, the costotransverse ligament, and the pleura. If the pleura is visualized at a depth of 4 cm or less, a linear probe oscillating at 8 to 12 MHz may be used (Fig. 37.3).
Once the anatomical structures are clearly identified, the skin is disinfected and anesthetized with 1% lidocaine using a 25G, 3.75-cm needle at the site of introduction of the block needle. The probe is covered by a sterile cover and repositioned in a sagittal plane in search of the initial anatomic landmarks (Fig. 37.4). The midpoint of the transducer is aligned mid way between the two adjacent transverse processes. A Tuohy needle, connected to an extension tube, is inserted at the cephalad or caudal extremity of the transducer using an in-plane technique (Fig. 37.5). The needle is directed deep to the costotransverse ligament and superficial to the pleura (Fig. 37.6). The paravertebral space is entered midway between the two transverse processes, avoiding bony contact. After negative aspiration for blood, 3 to 5 mL of local anesthetic is injected slowly into the paravertebral space. This results in a slight anterior displacement of the pleura (Fig. 37.7). Multiple levels may need to be injected if the local anesthetic volume is limited to 3 to 5 mL and if surgical anesthesia is required. For postoperative analgesia, some practitioners prefer to inject a high volume of
 Microanatomy of the Peripheral Nervous System and Stimulation Thresholds Inside and Outside the Epineurium
Microanatomy of the Peripheral Nervous System and Stimulation Thresholds Inside and Outside the Epineurium
 Ultrasound-Guided Intraneural Injection—The Human Data
Ultrasound-Guided Intraneural Injection—The Human Data
 Ultrasound-Guided Blocks at the Elbow and Forearm
Ultrasound-Guided Blocks at the Elbow and Forearm
 Ultrasound-Guided Distal Parasacral Block
Ultrasound-Guided Distal Parasacral Block
 Fundamentals of Ultrasound-Guided Pediatric Regional Anesthesia
Fundamentals of Ultrasound-Guided Pediatric Regional Anesthesia
 Ultrasound-Guided Genitofemoral Nerve Block
Ultrasound-Guided Genitofemoral Nerve Block




Related posts:
Microanatomy of the Peripheral Nervous System and Stimulation Thresholds Inside and Outside the Epineurium
Ultrasound-Guided Intraneural Injection—The Human Data
Ultrasound-Guided Blocks at the Elbow and Forearm
Ultrasound-Guided Distal Parasacral Block
Fundamentals of Ultrasound-Guided Pediatric Regional Anesthesia
Ultrasound-Guided Genitofemoral Nerve Block
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
