ULTRASOUND: BASICS
ESSENTIAL CONCEPTS
Ultrasound imaging uses the pulse-echo principle in which a short burst of sound waves are emitted from a transducer and directed to the underlying tissue. Diagnostic ultrasound uses sound waves of frequencies between 2 and 20 MHz. When a sound beam is directed toward the body, tissue reflects, absorbs, or scatters the beam. Each of these responses determines the nature of the received signal. The sum of acoustic energy losses from absorption, scattering, and reflection is called attenuation.
Reflection is a result of the passage of sound between tissues with different acoustic impedances, i.e., resistance. Absorption, meanwhile, is directly proportional to ultrasound frequency and determines resolution, or the ability to differentiate between adjacent structures. Resolution can be separated into two dimensions, parallel to and across the beam. Depth resolution is a function of length of the ultrasound pulse, and near-surface resolution implies distinguishing between superficial reflectors. The ability of ultrasound to detect reflectors at a certain depth is called sensitivity. A more sensitive system detects more intense reflection signals1–4 (Figure 2–1).
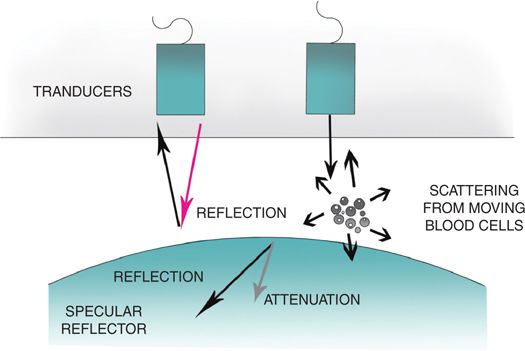
Figure 2–1 Schematic depicting the reflection, scattering, and absorption of ultrasound waves.
There are two types of ultrasound imaging commonly used today:
1. B-mode, which is a two-dimensional grayscale imaging. Images are dependent on amplitude information from sound beams passing through, or reflecting from, tissue.
2. M-mode in which the intensity of the backscattered beam is represented as pixel brightness. The image produced is the result of the compilation of different scan lines, each produced by a single pulse-echo. Thus the image will have high temporal resolution, which is essential in cardiac assessments.5–8
INTERPRETATIVE PRINCIPLES
Anatomy seen on ultrasound imaging is described in terms of morphology, which consists of external contour (boundaries and shapes) and internal echo pattern (in practical terms, brightness). Contour of a structure also describes its margins. When an organ has a well-defined margin it is usually due to the presence of a capsule, showing a sharp margin around the less echogenic parenchyma.
Internal echo pattern is described by the echogenicity—or ability to reflect sound waves—of a structure relative to its surrounding structures. For example, a lesion that is more echogenic, or hyperechoic, will be brighter than the surrounding structures (Figures 2–2 through 2–4). If structures contain lower echoes, they will be hypoechoic or echopenic and will appear darker (Figures 2–5 and 2–6). A lesion without echoes, such as a renal cyst containing simple fluid, is anechoic or sonolucent, and will appear completely black.
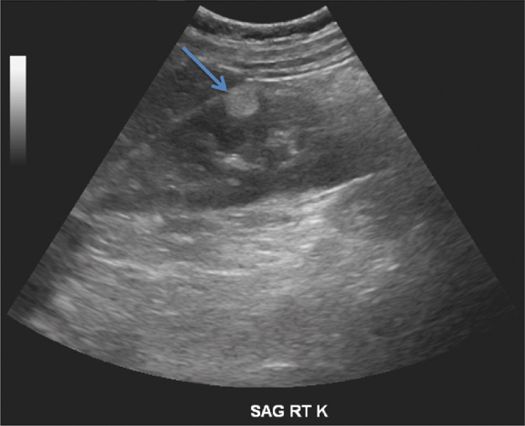
Figure 2–2 Angiomyolipoma (arrow) of right kidney, seen as a hyperechoic (bright) mass.
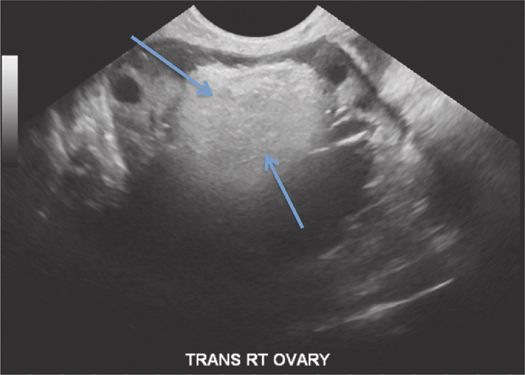
Figure 2–3 Hyperechoic mass. Dermoid cyst, in this case arising from the right ovary.
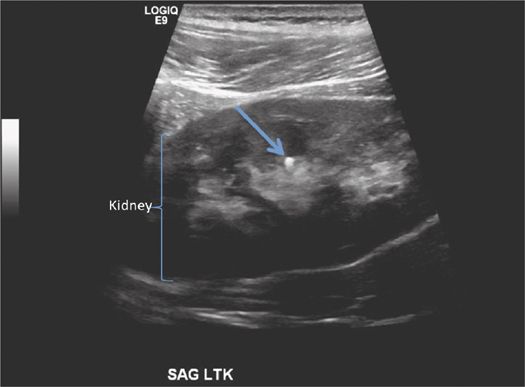
Figure 2–4 Calculus (arrow) in inter-polar region of the right kidney, depicted as a hyperechoic focus.
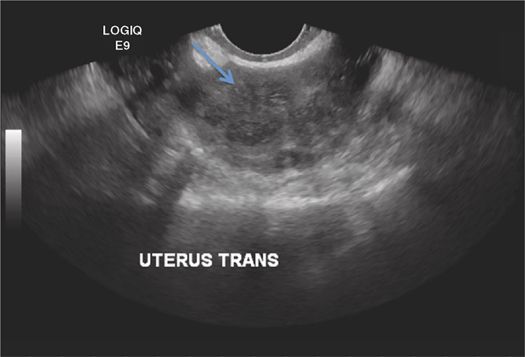
Figure 2–5 Transvaginal ultrasound showing ovarian fibroid (arrow), depicted as a well-defined hypoechoic lesion. Note its dark appearance relative to the surrounding tissue.
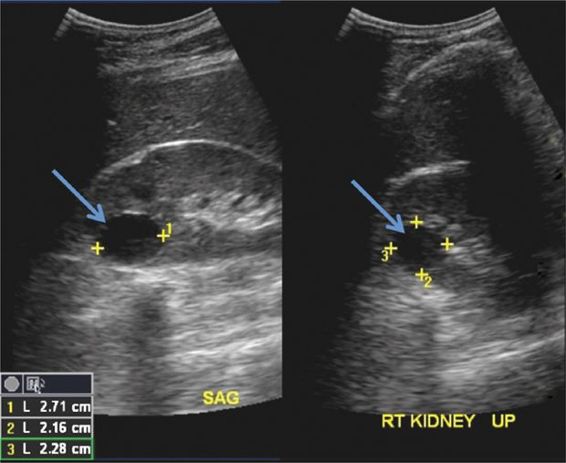
Figure 2–6 Transabdominal ultrasound scan showing simple cyst (arrow) in the right kidney. Note the anechoic (black) appearance, and the sharp, smooth borders, classic for a cyst.
Echo pattern can also be described by its homogeneity. A heterogeneous mass on ultrasound, for example, contains both hyperechoic and hypoechoic areas (Figure 2–7). In contrast, a homogeneous mass contains a uniform distribution of either hyperechoic or hypoechoic areas (Figure 2–8).
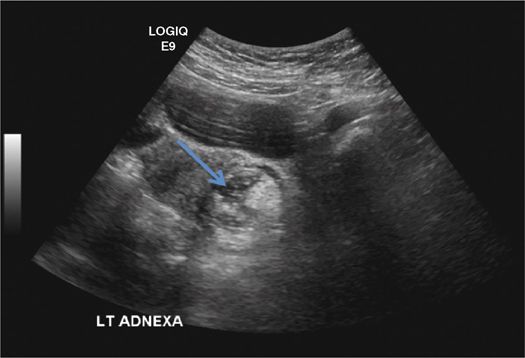
Figure 2–7 Transabdominal ultrasound showing hetergeneous lesion (arrow) in the left adnexa, with both hyperechoic and hypoechoic components. Workup confirmed a dermoid cyst.
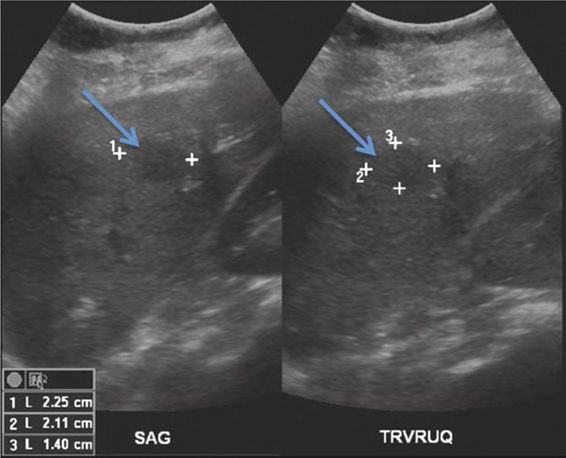
Figure 2–8 Transabdominal liver ultrasound in this patient with breast carcinoma showing a homogeneous, hypoechoic liver lesion (arrows). Biopsy confirmed a hepatic metastasis.
A highly attenuative or hyperattenuating mass poorly transmits echoes. High attenuation is the result of scattering, reflecting, or absorbing the sound waves. Increased attenuation will result in a hypoechoic, solid-appearing mass. In contrast, if a sound beam passes through a medium unimpeded, we see enhanced transmission, or posterior acoustic enhancement behind the lesion, organ, or mass.
The reflecting surface (tissue) determines the type of echo that is reflected back to the ultrasound probe and can be divided into two types:
1. Simple cystic structures are usually smooth walled and have well-defined borders (Figure 2–9). The fluid within cysts is homogeneous and thus lacks any acoustic interface. The result is an anechoic image with clear, smooth borders. Cystic masses are also characterized by lack of attenuation of the adjacent structures, which appear enhanced through transmission. A predominantly cystic structure is termed complex if it contains septations, debris, or solid elements1,5–8 (Figure 2–10).
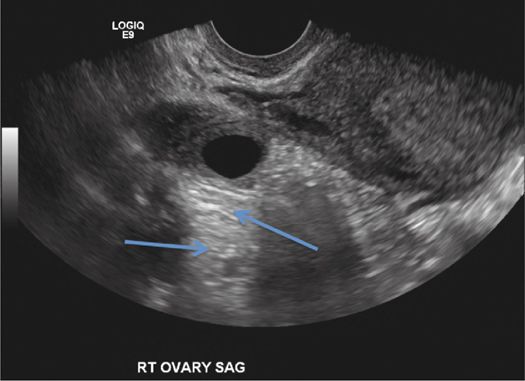
Figure 2–9 A zone of posterior enhancement (arrows) underneath a simple ovarian cyst.

Figure 2–10 Transvaginal ultrasound showing complex cyst (arrow) with irregular contour in the right ovary.
2. In contrast, solid structures have a multitude of acoustic interfaces. Some solid structures present with very homogeneous, low-amplitude internal echo patterns that can mimic cystic structures, e.g., enlarged lymph nodes caused by lymphoma. However, in principle solid structures have more complex echo patterns appearing either hyper- or hypoechoic and in general can be quite heterogeneous.
As previously stated, evaluation of any structure, cystic or solid, requires characterization of the structural contour, echo pattern, and attenuation.
IMAGE OPTIMIZATION
 Transducer Choice
Transducer Choice
Selecting the right ultrasound probe is essential to acquire optimal images, although at times more than one probe may be appropriate for a given exam. As a general rule, high-frequency probes are best for superficial structures (7- to 15-MHz frequencies for thyroid, scrotal, and musculoskeletal scans). Lower frequency probes ranging from 2 to 5 MHz are best for abdominal, pelvic, and obstetric scans because they permit deeper penetration.
Three basic types of probes used in bedside point-of-care ultrasound are linear, curvilinear, and phased array. Linear (vascular) probes have higher frequency and are more suitable for imaging superficial structures and vessels. Curvilinear probes may have a wider footprint and lower frequency for abdominal ultrasound, or may be arranged in a tighter array (giving a wider field of view) and higher frequency intended for endocavitary ultrasound (e.g., transvaginal). Phased-array probes can be used to image the area between ribs. The generated images differ between transducers: curvilinear and phased-array probes yield images that are pie shaped (narrow in the near field and wider in the far field), whereas linear probes produce rectangular images.9,10
Table 2–1 summarizes maneuvers to optimize image quality with ultrasound.







