A detailed transesophageal echocardiographic (TEE) examination of the right-sided heart valves can provide accurate diagnosis of valvular diseases; define anatomic, functional, and perivalvular abnormalities; and guide appropriate management. Integration of this information with the evaluation of the cardiac chambers is necessary to assess the degree of the pathology and determine its impact on cardiac function. In a review of 1918 cases undergoing intraoperative TEE prior to cardiac surgery, discrepant findings at the time of surgical inspection were present in only 48 patients, of which five involved the tricuspid and pulmonic valves.1 Therefore, this modality should yield adequate diagnostic accuracy when the exam is conducted appropriately. This chapter discusses the main pathologies involving the tricuspid and pulmonic valves leading to regurgitation and/or stenosis, and their assessment by two-dimensional TEE (Table 10–1). Even with the advent of three-dimensional matrix array probes allowing the acquisition of real-time images, optimal visualization of the tricuspid and pulmonary valves is seldom feasible2; therefore, their three-dimensional evaluation will depend on future improvements of this technology.
Tricuspid Valve | Pulmonic Valve | |||
|---|---|---|---|---|
Regurgitation | Stenosis | Regurgitation | Stenosis | |
Congenital | ||||
Predominant leaftlet problem | ||||
Prolapse | + | |||
Congenital stenosis | + | + | ||
Ebstein anomaly | + | |||
Dysplasia | + | + | + | + |
Cleft leaflet | + | |||
Predominant annulus problem | ||||
Marfan syndrome | + | + | ||
Acquired | ||||
Predominant leaftlet problem | ||||
Endocarditis | + | + | + | + |
Rheumatic heart disease | + | + | + | + |
Carcinoid heart disease | + | + | + | + |
Hypereosinophilic syndrome | + | + | ||
Radiation therapy | + | + | ||
Drugs (Fen-Phen, methysergide) | + | +/− | ||
Predominant annulus problem | ||||
Pulmonary hypertension | + | + | ||
Other | ||||
Trauma | + | + | ||
Right ventricular infarction | + | |||
Tumor (eg, myxoma) | + | + | ||
The tricuspid valve, the largest of the four cardiac valves, lies slightly below the plane of the mitral valve, and is in close proximity to the aortic valve. The three leaflets of the tricuspid valve are named anterior, posterior (inferior), and septal (medial) based on their relative positions (Figure 10–1). The septal leaflet’s insertion point at the septum is more apically displaced than that of the anterior mitral leaflet. The two major papillary muscles, the anterior and posterior, are located on the corresponding walls of the right ventricle. Through their chordae tendineae, they attach to the anterior and posterior cusps, and the posterior and septal cusps, respectively. When present, a smaller septal papillary muscle attaches to the septal and anterior cusps.3 The three leaflets of the valve can be imaged using different angulations of the imaging plane together with flexion of the probe tip (see Figure 10–1).
Figure 10-1.

Schematic diagram of the heart that shows the spatial relationships of the valves. Note that the aortic valve plane is almost perpendicular to that of the pulmonic valve, so that when the imaging plane is along the short axis of the aortic valve (imaging at 60°, shaded triangle), the pulmonic valve is imaged in its long axis. When imaging at 0° to obtain the four-chamber view (solid straight lines), anteflexion and retroflexion will move the imaging plane anteriorly and posteriorly to allow imaging of the anterior and posterior leaflets of the tricuspid valve, respectively. (A, anterior;P, posterior; S, septal; L, left; R, right.)
From the midesophageal four-chamber view, rightward rotation of the probe can help position the tricuspid valve in the center of the image. This view will show the septal leaflet to the right of the display and the nonseptal (anterior or posterior) leaflet to the left of the display, depending on the amount of anteflexion or retroflexion of the probe (Figure 10–2).

Starting from the midesophageal four-chamber view, rotating the angle forward to approximately 60° will yield a cross-sectional view of the aortic valve, with a transverse section of the right ventricular inflow and outflow tracts. Slight turning of the probe to the right might be needed for better visualization of the structures. In this view, the anterior leaflet of the tricuspid valve is seen next to the aortic valve. The posterior leaflet of the tricuspid valve is seen to the left of the display attached to the right ventricular wall (Figure 10–3).

Turning the probe to the right in the transgastric short-axis view of the left ventricle will bring the right ventricle to the center of the display. A long-axis view of the right ventricle is then obtained by rotating the multiplane angle to about 120°. The chordae tendineae and papillary muscles are well seen, since they are perpendicular to the ultrasound beam. In this view, the posterior leaflet of the tricuspid valve is visualized in the near field, attached to the inferior wall, while the anterior leaflet is located in the far field, attached to the anterior wall of the right ventricle (Figure 10–4).

Starting from the transgastric right ventricular inflow view, the tricuspid annulus is centered in the image by slightly withdrawing the probe. Rotating the angle back to about 30° will generate a short-axis view of the tricuspid valve. The septal leaflet is visualized to the right of the display. The anterior and posterior leaflets are seen in the left-sided far and near fields, respectively (Figure 10–5).

Trivial or very mild degrees of tricuspid regurgitation can frequently be present in normal individuals, and in the absence of abnormalities of the valvular structures or cardiac chambers, it should be regarded as a normal variant. Pathologic tricuspid regurgitation can be either congenital or acquired. Ebstein’s anomaly is one of the important causes of congenital tricuspid regurgitation, and echocardiography plays a major role in the diagnosis and surgical planning. More commonly, however, tricuspid regurgitation is the result of right ventricular dilatation and/or dysfunction secondary to pulmonary hypertension or right ventricular infarction. Rheumatic heart disease (less frequently encountered in developed countries) and carcinoid heart disease result in thickening, restricted mobility, and/or malcoaptation of the leaflets, leading to incompetence of the valve. In patients with endocarditis, vegetations that tend to form on the atrial surface of the leaflets can lead to destruction of the leaflets and/or chordae, causing significant degrees of regurgitation in advanced cases. Annular dilatation can be seen in some cases of Marfan’s syndrome, and tricuspid valve prolapse with or without associated mitral valve prolapse is another cause of tricuspid regurgitation. Occasionally, tumors such as right atrial myxomas can interfere with the normal coaptation of the leaflets, therefore causing regurgitation.
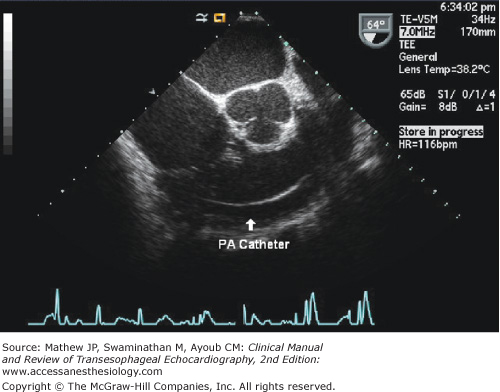
Two-dimensional examination of the tricuspid valve apparatus provides significant information regarding the underlying cause and mechanism of tricuspid regurgitation. The identification of anatomic abnormalities (eg, Ebstein’s anomaly), abnormal masses, annular dilatation, and noncoaptation (see Figure 10–3) are all essential to make a correct diagnosis. Pacemaker wires or catheters passing through the tricuspid orifice are readily visualized (Figure 10–6), and although uncommonly encountered with the right-sided valves,4 TEE is highly sensitive for the detection of vegetations.5 Movement of any of the leaflets beyond the plane of the tricuspid annulus inside the right atrium indicates the presence of tricuspid prolapse (Figure 10–7).6 Additionally, in patients with tricuspid valve prolapse, the leaflets and chordae are usually redundant and myxomatous. Features characteristic of Ebstein’s anomaly include apical displacement or “off-setting” of the hinge point attachment of the septal leaflet relative to that of the anterior mitral leaflet. A displacement index is easily produced by measuring the distance between the two hinge points and indexing to body surface area. This can be done in the midesophageal four-chamber view, and different angulations of the probe will help obtain the maximal difference. An indexed value greater than 8 mm/m squared7,8 or a nonindexed value of greater than 15 mm in children and 20 mm in adults,9 together with elongation of the anterior leaflet (the so-called “sail-like” or “curtain-like” appearance),10,11 tethering, and restricted leaflet motion,7 distinguish this congenital anomaly from other causes of tricuspid regurgitation. Additional echocardiographic features of Ebstein’s anomaly include apical displacement of the other leaflets, absence or fenestration of any of the leaflets, and “atrialization” of a part of the right ventricle.

Carcinoid heart disease in patients with carcinoid syndrome results from fibrous deposits on the endocardium of the right-sided valves and chambers. This leads to thickening and rigidity of the leaflets, with the valves fixed in an open position, and associated stenosis is common. Involvement of the left-sided valves should prompt a careful evaluation for right-to-left shunting.12 Thickening, shortening, and restricted mobility of the leaflets are all characteristics of rheumatic involvement of the valve. The presence of malcoaptation of the leaflets usually indicates severe regurgitation, as does a large tricuspid annulus (>2.1 cm/m2 of body surface area).13 Although measurement of the tricuspid annulus should be performed in multiple views during diastole, using the frame that shows maximal distance between the insertion points of the leaflets, the measurement from the transgastric right ventricular (RV) inflow view correlates best with surgical measures.14 Moreover, the dimensions of the right-sided chambers can provide clues to the severity of regurgitation. In contrast to mild regurgitation, chronic moderate and severe tricuspid regurgitation are usually associated with a dilated right atrium and ventricle. This is, however, not true in cases of acute moderate or severe tricuspid regurgitation where the chambers do not have time to remodel.
Color Doppler mapping can detect and provide a degree of quantification of the severity of tricuspid regurgitation. When applied, the multiplane angle should be changed and the probe tip manipulated in order to demonstrate the largest possible jet of regurgitation (Figure 10–8). Doppler principles similar to those used in the assessment of mitral regurgitation can be used to assess tricuspid regurgitation (Table 10–2). Measuring the vena contracta, which is the narrowest portion of the jet at the orifice of the valve, is easy to perform in the midesophageal four-chamber view; the cutoff for severe regurgitation is considered to be7 mm.15,16 In centrally directed regurgitation, measurement of the jet area can be helpful; an area of greater than 10 cm2 is indicative of severe insufficiency.16 Doppler parameters that indicate increased severity of tricuspid regurgitation include a tricuspid inflow velocity higher than 1 m/s, and a dense, triangular, and early-peaking continuous-wave (CW) Doppler signal of the tricuspid valve. The proximal isovelocity surface area (PISA) method can be applied for more quantitative assessment (Figure 10–9). A simplified approach has been suggested, whereby measuring the PISA radius at a Nyquist limit of about 28 cm/s can provide an estimate of the severity of the regurgitation; a radius of 5 mm or less usually identifies mild degrees, and a radius greater than 9 mm is found in severe cases.16

Regurgitation Severity | |||
|---|---|---|---|
Mild | Moderate | Severe | |
Two-dimensional findings | |||
Leaflet morphology | Usually normal | Can be normal | Abnormal |
Leaflet coaptation | Normal | Malcoaptation ± flail | |
Right-side chambers | Usually normal | Can be normal | Dilated (unless acute) |
Tricuspid annulus diameter | >2.1 cm/m2 | ||
Doppler findings | |||
Area of the jet (cm2)a,b | <5 | 5-10 | >10 |
Vena contracta width (mm)b | >7 | ||
PISA radius (mm)c | ≤5 | 6-9 | >9 |
CW Doppler signal | Soft and parabolic | Dense, variable contour | Dense, triangular with early peaking |
Coronary sinus flow | Forward in systole | Systolic reversal | |
Hepatic venous flow | Systolic dominance | Systolic blunting | Systolic reversal |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


