(1)
University of Maryland Medical Center, Baltimore, MD, USA
(2)
University of Maryland School of Medicine, Baltimore, MD, USA
Keywords
TraumaExternal genitaliaUrethraPriapismPenile fracturePenile implantArtificial urinary sphincterTraumatic Injuries
Amputation
Penile amputation is usually the result of self-inflicted injury or mutilation (Fig. 16.1). Psychiatric evaluation should be considered in all cases given the high rate of comorbid underlying psychiatric illness. Ideally, the severed portion of the penis should be wrapped in saline-soaked gauze and double-bagged in ice. Reanastomosis is possible with a cold ischemia time of up to 16 h or warm ischemia up to 6 h. If the severed piece is unavailable, a penile stump should be created in a similar fashion to a distal penectomy with corporal closure and formation of a spatulated urethral neomeatus. A microvascular approach to reattachment yields significantly greater functional and sensory outcomes as compared to a strictly macrovascular approach. However, either technique yields satisfactory erectile function in greater than 50 % of cases. Loss of sensation, skin necrosis, and urethral stricture can also occur as a result of the amputation or repair, and such complications are more common after macrovascular repair. Adjuvant therapy to surgical reattachment includes hyperbaric oxygen treatment and leeches to encourage healing and blood flow [1, 2].

Fig. 16.1
Traumatic amputation of the penis.
Zipper Injury
Zipper injury is most commonly encountered in the adolescent and adult inebriated population. Before manipulation, lubrication and a penile block should be administered. A single attempt at unzipping the retained skin should be performed before further intervention. Cutting the cloth in between each of the zipper teeth may release the entrapped portion of the penis. Using a bone cutter to sever the median bar of the zipper may also allow for release [1].
Constricting Devices
The most common causes for strangulation injury are hair, rubber band, and string-related constriction. As the majority of cases are seen in children, child abuse should always be considered. In the adult population, strangulation is often a result of sexual practices. Patients will typically present with penile edema and voiding symptoms from an either visible or non-visible source (i.e., hair). Presentation may be delayed due to patient embarrassment. Initial management should be aimed at decompression of the penis. Adequate lubrication should be administered before attempted direct removal of the constricting device. A distal tourniquet or glandular puncture can be utilized in an attempt to decrease swelling. Consider suprapubic tube placement if the patient is unable to void for an extended period of time. Plastic and nonmetal devices can be excised with a scalpel or cast saw. Removal of metal objects may require the use of industrial-strength equipment with the patient under anesthesia. Prolonged constriction may lead to skin necrosis requiring possible reconstruction with skin grafts [1].
Penetrating Injuries
Gunshot wounds account for most penetrating injuries to the penis. Up to 80 % of cases present in the context of major injury to surrounding structures such as the abdomen, pelvis, and lower extremity [3]. Potentially fatal injuries must be searched for and treated prior to exploration of the genitalia. Almost all penetrating penile injuries require surgical exploration. Immediate management often leads to an excellent prognosis. Exploration with extensive irrigation, removal of foreign material, and debridement of necrotic tissue with added antibiotic prophylaxis can lead to good functional and cosmetic results. The most common approach is through a circumcising incision in which the penis is degloved to provide optimal exposure [4]. Absorbable sutures are used to repair injuries to the corpora. Nonviable tissue is removed, the tunica albuginea is closed tightly, and the overlying skin is then loosely closed. An artificial erection can be used to detect any penile curvature that may result from the repair of a corporal injury. Plication techniques can then be used to straighten the erect penis. Other potential complications include sexual and voiding dysfunction.
Up to 50 % of penile gunshot wounds will have associated urethral injury [4]. Blood at the meatus, voiding difficulty, or obvious injury near the urethra are indications that retrograde urethrography and/or intraoperative cystoscopy should be performed to evaluate for urethral injury. Absence of blood at the meatus can be misleading, and urethral damage may still be present. In the setting of urethral injury, primary closure is possible via standard urethroplasty with great functional outcomes. In cases of more extensive injury, suprapubic catheter placement and staged urethroplasty may be necessary [1].
Testicular Trauma
The testes are subject to both blunt and penetrating trauma. Blunt trauma is more common and is most often related to sports injury, motor vehicle accidents, and assault. Penetrating trauma can result in bilateral injury involving adjacent structures which typically requires surgical exploration (Fig. 16.2). Regardless of suspected bullet trajectory or physical findings, both testes should be explored [1].
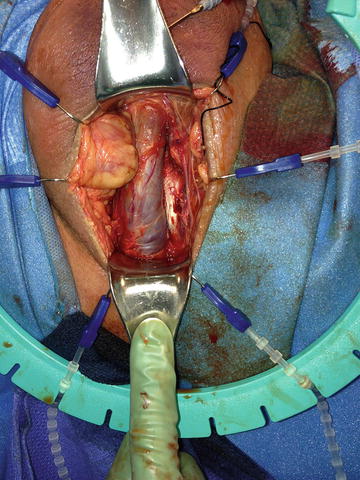
Fig. 16.2
Penetrating trauma to the scrotum.
Differential diagnosis considerations for testicular trauma include hematoma, torsion (Fig. 16.3), fracture, and dislocation. Initial workup of blunt testicular trauma should include physical examination and ultrasound. Although edema and ecchymosis are commonly seen, these findings do not necessarily correlate with the degree of underlying injury to the testicle. Ultrasound can be used to evaluate vascular integrity and for testicular fracture. Heterogeneous echogenicity of the testes is diagnostic of fracture. If ultrasound results are equivocal, surgical exploration should be performed emergently based on physical exam findings alone and should not be delayed. Management is aimed at salvage of viable testicular tissue. Nonviable tissue is debrided and the tunica albuginea is closed primarily. If the defect is too wide, a free graft of tunica vaginalis can be used [5]. Even in the absence of proven fracture, large intratesticular hematomas and hematoceles should be managed operatively. Drainage of the hematoma has been shown to prevent pressure necrosis and delayed orchiectomy. In addition, 80 % of significant hematoceles are caused by underlying testicular rupture. Delaying surgical exploration and testicular salvage for greater than 3 days significantly increases the morbidity associated with the trauma. Potential complications of conservative nonoperative management include infection, necrosis, chronic pain, and delayed orchiectomy. Ruptured testes that were explored before 72 h have a salvage rate of 90 % compared to 45 % of those explored beyond that window [1].

Fig. 16.3
Testicular torsion.
Common Surgical Emergencies
Although not necessarily traumatic in origin, both priapism and infections of the external genitalia may require emergent surgical intervention and are therefore worthy of further discussion.
Priapism
Priapism is a full or partial erection that continues more than 4 h beyond sexual stimulation and orgasm or is unrelated to sexual stimulation. There are two types of priapism: ischemic (low-flow) and nonischemic (high-flow, arterial) priapism.
Nonischemic (high-flow) priapism is caused by unregulated cavernous arterial inflow resulting in a non-painful and partially rigid erection which is not associated with hypoxia or acidosis and does not require emergent intervention. Nonischemic priapism is most commonly traumatic in origin, often resulting from a straddle injury or pelvic fracture that leads to disruption of a cavernous artery. High-flow priapism can develop immediately following trauma or days later, and Doppler ultrasound can usually identify a cavernosal artery fistula. Treatment is not an emergency, and approximately 62 % of cases will resolve without intervention.
In contrast to nonischemic priapism, ischemic or low-flow priapism requires emergent surgical intervention aimed at detumescence and the preservation of erectile function. Ischemic priapism is a persistent erection marked by rigidity of the corpora cavernosa and little or no cavernous arterial inflow which results in progressive hypoxia, acidosis, and a painful, fully rigid erection. On examination, both the glans and corpus spongiosum are soft, and the corporal bodies are rigid and tender to palpation. Left untreated, resolution may take days, and interventions beyond 48–72 h may help to relieve pain but will have little benefit in preserving erectile function.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


