Trauma
17-1 Basilar Skull Fracture
Madelyn Garcia
Clinical Presentation
Signs and symptoms of basilar skull fracture vary depending on the area involved. Anterior fossa fractures are often accompanied by facial injury, cerebrospinal fluid (CSF) rhinorrhea, or bilateral periorbital ecchymosis.1 Patients with middle fossa fractures present with postauricular hematoma (Battle’s sign), hemotympanum, otorrhea, facial nerve palsy, vertigo, tinnitus, or hearing loss.1 Those with posterior fossa fractures through the occipital bone may present with swallowing and airway difficulties secondary to glossopharyngeal and vagal nerve injury, or with mental status changes from associated epidural hematoma.1
Pathophysiology
Basilar skull fractures are associated with deceleration injuries involving head strikes on hard surfaces.1
Diagnosis
Management
In conjunction with advanced trauma life support (ATLS) protocols, early neurosurgical, maxillofacial, or otolaryngology consultation should be considered. Expanding hematomas need to be evacuated immediately. Orbital nerve compression may require decompression and high-dose steroids. CSF leak should be surgically closed by repair of the tear in the dura, and vascular injuries may be repaired or conservatively watched with repeat CT scanning.1
REFERENCES
1. Samii M, Tatagiba M. Skull base trauma: diagnosis and management. Neurol Res 2002;24:147-156.
2. Stone JA, Castillo M, Neelon B, Mukherji SK. Evaluation of CSF leaks: high resolution CT compared with contrast enhanced CT and radionuclide cisternography. Am J Neuroradiol 1999;20:706-712.
3. Dahiya R, Keller JD, Litofsky NS, et al. Temporal bone fractures: otic capsule sparing versus otic capsule violating clinical and radiographic considerations. J Trauma 1999:47:1079-1083.
17-1 Basilar Skull Fracture
Madelyn Garcia
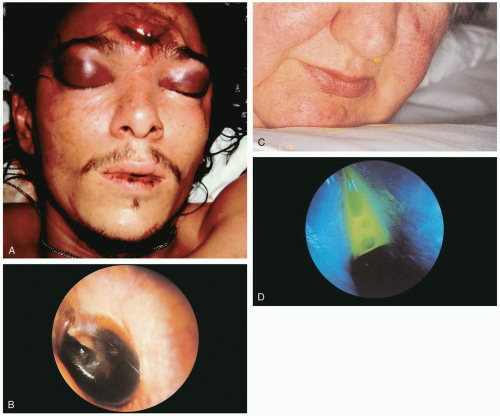 FIGURE 17-1 A: “Raccoon’s eyes.” (Courtesy of Michael Greenberg, MD.) B: Hemotympanum. The older, dark-brown, bloody fluid in this right middle ear has colored the tympanic membrane black. (From Benjamin, with permission.) C: The fluorescein test for cerebrospinal fluid (CSF) rhinorrhea. In this positive test, fluorescein-stained CSF is seen dripping from the patient’s left nostril after 45 minutes. (From Benjamin, with permission.) D: CSF rhinorrhea. With blue light, fluorescence is induced and the CSF shines with a neon-like color. The fluorescein was followed into the sphenoethmoidal recess, close to the sphenoid sinus ostium. (From Benjamin, with permission.) |
17-2 Skull Fracture
Madelyn Garcia
Clinical Presentation
Patients with skull fracture present after head trauma. Signs and symptoms vary, depending on the type of fracture and associated injuries such as intracranial hemorrhage.1
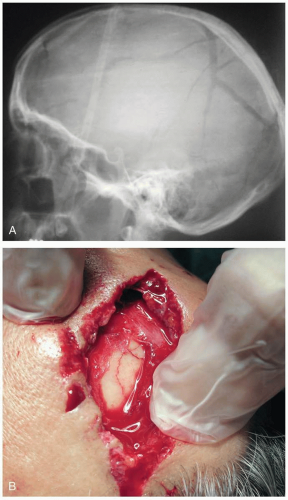 FIGURE 17-2 A: Radiograph showing severely comminuted skull fracture. (Courtesy of Michael Greenberg, MD.) B: A skull fracture is clearly visible in the base of this scalp. (Courtesy of Anthony Morocco, MD.) |
Pathophysiology
Linear skull fractures go through the entire thickness of the skull and occur most often in the temporal-parietal and frontal regions. They are the most common type of skull fracture.1 Depressed skull fractures have a bony segment that is displaced inward. These fractures are considered significant if the fragment is depressed below the inner table of the adjacent calvaria, or if the fracture overlies an important structure such as a venous sinus or the motor or sensory cortex.1 In open skull fractures, the dura has been exposed. Open fractures can occur if a scalp laceration overlies the fracture site or if the paranasal sinuses or middle ear structures are disrupted, allowing communication between the brain and the environment.1
Diagnosis
Skull fractures may be suspected based on the history and physical examination, but usually radiographic confirmation is required. Computed tomographic (CT) scanning is the diagnostic modality of choice. Plain films are helpful in detecting linear skull fractures, which may be missed if they run in the same plane as the CT slices.1
Clinical Complications
Complications include intracranial hemorrhage, meningitis, cerebrospinal fluid leakage, abscess formation, leptomeningeal cyst, seizures, epilepsy, and future neuropsychological dysfunction.2
Management
It is essential to exclude underlying intracranial injury, which is up to four times more common in the presence of a skull fracture. Linear, closed skull fractures are treated symptomatically, whereas open fractures should be treated with antibiotics and tetanus toxoid.1 Depressed skull fractures are considered “high-risk” and require close observation.1 Intraoperative washout and fragment elevation should be considered on a case-bycase basis. Seizure prophylaxis is controversial but is recommended in the immediate postinjury period.2 Neurosurgical consultation should be considered for all skull fractures.1,2
REFERENCES
1. Levine RS, Grossman RI. Head and facial trauma. Emerg Med Clin North Am 1985;3:447-473.
2. Annegers JF, Coan SP. The risks of epilepsy after traumatic brain injury. Seizure 2000;9:453-457.
17-3 Scalp Laceration
Dante Pappano
Clinical Presentation
Patients with scalp lacerations present with a history of trauma and obvious disruption of the scalp dermis and epidermis.
Pathophysiology
The scalp is a common site for lacerations, which may result from either blunt or sharp/penetrating mechanisms, or as a consequence of a bite.1,2 The distinction is important, because lacerations caused by crushing rather than cutting forces often generate more devitalized tissue, with a higher probability of wound infection. Those lacerations caused by bites are often contaminated by bacteria and may represent the greatest risk for infection.1
 FIGURE 17-3 Complex scalp laceration with laterally based flap. (Courtesy of Andrew Liteplo, MD.) |
Diagnosis
Diagnosis is based on physical findings; however, the extent of injury may not be clear until the wound area has been anesthetized, cleansed, and thoroughly inspected.1
Clinical Complications
Extensive hemorrhage may lead to hypotension. Wound infection, substantial scalp tissue loss, dehiscence, and poor cosmesis are potential complications. Retained foreign bodies may serve as a nidus for infection.
Management
Direct pressure to control hemorrhage is usually effective. Hemostasis may be difficult to attain due to the vascularity of the scalp. Persistent bleeding may be controlled in part by infiltration of vasoconstrictive agents and recompression of the wound. In preparing the field for closure, most authorities agree that the hair along the wound edge should be cut short but not shaved.1,2 Once the defect is ready to be repaired, the physician must select among multiple techniques of wound closure, including standard suturing or stapling and less common alternatives such as hair tying and the hair apposition technique (HAT).3
REFERENCES
1. Hollander JE, Singer AJ. Laceration management. Ann Emerg Med 1999;34:356-367.
2. Howell JM, Morgan JA. Scalp laceration repair without prior hair removal. Am J Emerg Med 1988;6:7-10.
3. Hock MO, Ooi SB, Saw SM, Lim SH. A randomized controlled trial comparing the hair apposition technique with tissue glue to standard suturing in scalp lacerations (HAT Study). Ann Emerg Med 2002;40:19-26.
17-4 Diffuse Axonal Injury
Dante Pappano
Clinical Presentation
Diffuse axonal injury (DAI) is a form of traumatic brain injury that is characterized by immediate neurologic dysfunction with loss of consciousness and histologic evidence of axonal damage.1 The clinical hallmark of DAI is impairment of consciousness.
Pathophysiology
DAI is caused by acceleration/deceleration forces that result in shearing injury to axons and small blood vessels.1 Often there is associated injury related to anoxia, penetrating brain injury, intracerebral hemorrhage, or contusion. The primary axonal injury is a mechanical axotomy predominating in the brainstem, parasagittal white matter, and corpus callosum; however, secondary metabolic and neurotoxic stresses may lead to a wider area of damage.1,2
 FIGURE 17-4 “Diffuse axonal injury” is a term used to describe prolonged coma occurring after head trauma that is not caused by ischemia or a mass lesion. In this autopsy specimen, small hemorrhages are seen throughout the brain and corpus callosum. (From Jones, with permission.) |
Diagnosis
The diagnosis is presumptive based on clinical findings. Head computed tomography may demonstrate characteristic punctate hemorrhages but may be normal. Magnetic resonance imaging usually demonstrates acute signs of axonal shear injury.3 Definitive pathologic confirmation is available only at autopsy.1 In severe cases, coma may last several weeks or result in a persistent vegetative state.1
Clinical Complications
Death and persistent vegetative state are the most serious outcomes. Memory and cognitive impairment, balance problems, syndrome of inappropriate secretion of antidiuretic hormone (SIADH), diabetes insipidus, and hypopituitarism are also potential complications.1
Management
There is no specific therapy for primary axonal injury. Clinical trials with various neuroprotective agents are promising but have not yet been completed.2 Appropriate supportive care in the emergency department should be directed at decreasing secondary injury related to hypoxia and hypotension.2 Trauma surgery, neurosurgery, and neurology consultations usually are necessary.
REFERENCES
1. Meythaler JM, Peduzzi JD, Eleftheriou E, et al. Current concepts: diffuse axonal injury-associated traumatic brain injury. Arch Phys Med Rehabil 2001;82:1461-1471.
2. Bullock MR, Lyeth BG, Muizelaar JP. Current status of neuroprotection trials for traumatic brain injury: lessons from animal models and clinical studies. Neurosurgery 1999;45:207-217.
3. Hammoud D, Wasserman BA. Diffuse axonal injuries: pathophysiology and imaging. Neuroimaging Clin North Am 2002;12:205-216.
17-5 Cerebral Concussion
Dante Pappano
Clinical Presentation
Pathophysiology
Concussions result from head injuries associated with acceleration or deceleration forces applied to the brain.1 The exact mechanism of neuronal dysfunction is not clear, but mechanically induced depolarization followed by transmission abnormalities is likely.1 Structural injury to axons and blood vessels may also occur, but this may not fully explain the brief, temporary nature of the illness.
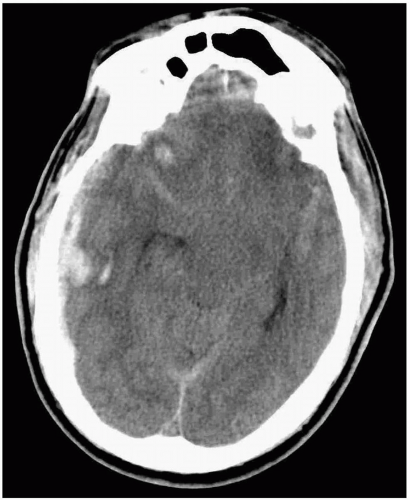 FIGURE 17-5 Computed tomogram showing evidence of intracerebral bruising. (Courtesy of Mark Silverberg, MD.) |
Diagnosis
The diagnosis is made clinically, often by history alone, because there may be no physical findings. There are three grades of injury. Grade 1 concussion involves anterograde amnesia lasting less than 30 minutes, with no loss of consciousness (LOC). Grade 2 injuries involve anterograde amnesia lasting up to 24 hours or LOC lasting less than 5 minutes. Grade 3 concussion demonstrates anterograde amnesia lasting longer than 24 hours or LOC lasting longer than 5 minutes. The neurologic examination may be normal or may demonstrate impairment of memory, concentration, or balance. Focal neurologic deficits are unusual.1,2
Clinical Complications
Complications include intracranial bleeding, “postconcussive syndrome,” seizures, or additive brain damage with multiple concussive episodes.2
Management
There is no specific treatment for a concussion. However, evaluation for other associated head and neck injuries is important. Additionally, if the concussion is related to sports, conservative advice regarding return to sports is necessary, because both brain and nonbrain injuries are more likely to occur when an athlete participates with less than optimal balance or concentration.1,2
REFERENCES
1. McCrory P, Johnston K, Mohtadi N, Meeuwisse W. Evidence-based review of sport-related concussion: basic science. Clin J Sports Med 2001;11:160-165.
2. Johnston K, McCrory P, Mohtadi N, Meeuwisse W. Evidence-based review of sport-related concussion: clinical science. Clin J Sports Med 2001;11:150-159.
17-6 Penetrating Head Injury
Michael Greenberg
Clinical Presentation
Patients with penetrating head injury (PHI) usually present with obvious penetrating injury inflicted by missiles, stab wounds, gunshots, or other penetrating objects. These injuries typically result from assaults, intentional self-harm, military- or warfare-related trauma, high-speed trauma, or industrial accidents.1,2
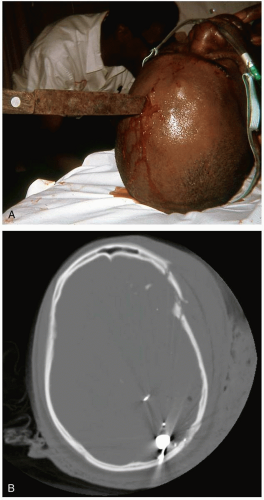 FIGURE 17-6 A: Stab wound to the head. (Courtesy of Michael Greenberg, MD.) B: Computed tomogram showing a gunshot wound to head. (Courtesy of Mark Silverberg, MD.) |
Pathophysiology
The extent and nature of PHI depends on the nature and extent of the wounding mechanism.
Diagnosis
The diagnosis of PHI is based on the history and clinical examination. Various adjunctive imaging studies, including computed tomography, magnetic resonance imaging, and angiography, may be needed to define the extent of injury.
Clinical Complications
Management
Patients should be assessed and stabilized in accord with the principles of advanced trauma life support (ATLS). Emergency, on-site neurosurgical consultation is essential in all cases of PHI. Intravenous antibiotics and tetanus prophylaxis should be provided in all cases, while the patient is still in the emergency department.1,2
REFERENCES
1. Bauer M, Patzelt D. Intracranial stab injuries: case report and case study. Forensic Sci Int 2002;129:122-127.
2. Brain Trauma Foundation. The American Association of Neurological Surgeons. The Joint Section on Neurotrauma and Critical Care. Trauma Systems. J Neurotrauma 2000;17:457-462.
17-7 Le Fort Fractures
Ellen Bass
Clinical Presentation
Le Fort fractures (LFFs) are associated with substantial facial edema that may obscure the underlying facial deformities. Malocclusion is often present, with the site of premature contact of the teeth helping to pinpoint the fracture site. Additionally, patients may have numbness of the upper lip, side of the nose, or upper gingiva if the infraorbital and superior alveolar nerves are disrupted.1 Diplopia may occasionally be present in type II or III Le Fort fractures.2
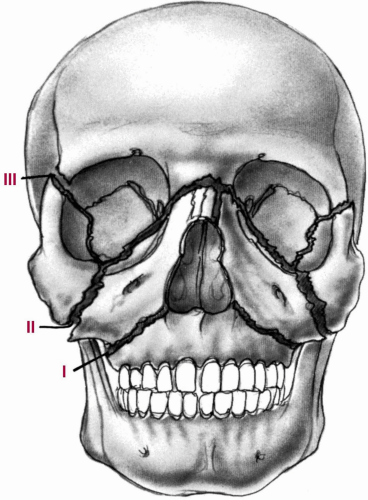 FIGURE 17-7 Le Fort fracture levels. Although these levels usually do not describe the extent or exact nature of midfacial fractures, they are still appropriately used for a general description of the injuries. (From Bailey, with permission.) |
Pathophysiology
The LFFs (types I, II, and III) are a series of midface fractures named after the French army surgeon, Dr. Rene Le Fort.2 Motor vehicle collisions, falls, and assaults are the major causes of LFFs.1 Forceful blunt trauma to the midface is the usual mechanism of injury. A LFF type I fracture is a horizontal fracture of the maxilla above the roots of the teeth. A LFF type II fracture extends more superiorly, through the infraorbital rim and over the nasal bones. A LFF type III fracture results in a separation of the maxilla, nasoorbitoethmoid complex, and zygomas from the cranial base.1
Diagnosis
A mobile mandible or midface found on physical examination should raise suspicion that an LFF exists. However, facial computed tomography is the imaging modality of choice to identify these injuries.1
Clinical Complications
Management
Airway control is of paramount importance because of the amount of facial edema and bleeding.1 All patients should receive a full trauma evaluation, and other life-threatening injuries should be investigated before the facial fractures are worked up. Consultation with an otolaryngologist or a plastic or oral surgeon is necessary, because these injuries require early operative repair with open reduction and internal fixation. Prophylactic antibiotics should be provided to cover oral and sinusdwelling microbes.1
REFERENCES
1. Ellis E 3rd, Scott K. Assessment of patients with facial fractures. Emerg Med Clin North Am 2000;18:411-448.
2. Patterson R. The Le Fort fractures: Rene Le Fort and his work in anatomical pathology. Can J Surg 1991;34:183-184.
17-8 Tripod Fractures
Jason Bell
Jacob W. Ufberg
Clinical Presentation
Tripod fractures are associated with blunt-force facial trauma. Patients present with facial pain and swelling. Patients may report anesthesia over the lower eyelid, upper lip, or side of nose; pain at the injury site with opening of the jaw; or diplopia.1
Pathophysiology
Tripod fractures include three points of separation: a fracture of the infraorbital rim, diastasis of the zygomatictemporal suture at the zygomatic arch, and disruption of the zygomatic-frontal suture in the lateral wall of the orbit.1 The three fracture lines may result in a free-floating, bony fragment that resembles a tripod. The zygoma may be displaced medially, inferiorly, and posteriorly, causing a depression deformity of the lateral face. Fracture at the infraorbital foramen may transect the infraorbital nerve, producing anesthesia. The lateral canthus of the eye is attached to the zygoma, which is pulled downward as the bone is displaced inferiorly, causing vertical dystopia and diplopia. The zygoma forms the roof of the maxillary sinus; when fractured, it may tear the mucosal lining, leading to epistaxis.2
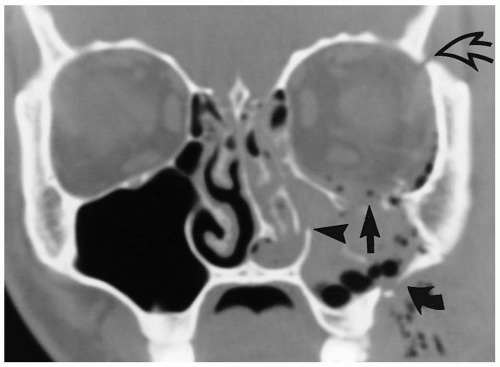 FIGURE 17-8 Comminuted, displaced fracture of the left zygomaticomaxillary complex (ZMC), as shown on coronal computed tomographic (CT) images from anterior to posterior. The CT scan shows disruption of the “friendly line” (curved arrow), the medial wall of the antrum (arrowhead), and the inferior orbital rim (arrow), as well as separation of the left zygomaticofrontal suture (curved open arrow). (From Harris and Harris, with permission.) |
Diagnosis
Physical examination may reveal facial asymmetry. Other common findings include lateral subconjunctival hemorrhage, periorbital ecchymosis, vertical dystopia, and epistaxis.2 A Water’s view radiograph serves as a screening radiograph for a suspected tripod fracture, based on history and physical examination findings. Abnormalities such as interruption of the cortex and soft-tissue clouding within the maxillary sinus, representing hemorrhage, may be clues to diagnosis.3 Patients with suspected tripod fractures should also receive axial and coronal computed tomography of the maxilla.1
Clinical Complications
Management
Patients with tripod fractures require emergency consultation and admission for surgical repair of the displaced fragments.2
REFERENCES
1. Ellis E 3rd, Scott K. Assessment of patients with facial fractures. Emerg Med Clin North Am 2000;18:411-448.
2. Hollier LH, Thornton J, Pazmino P, Stal S. The management of orbitozygomatic fractures. Plast Reconstr Surg 2003;111:2386-2392.
3. Keogh C, Torreggiani WC, Al-Ismail K, Munk PL. Musculoskeletal case 23: tripod fracture. Can J Surg 2002;45:279, 309-310.
17-9 Retrobulbar Hematoma
Ellen Bass
Clinical Presentation
Pathophysiology
Retrobulbar hematoma may accompany malar, orbital floor, Le Fort II, or Le Fort III fractures and may occur after blepharoplasty.1,2 Risk factors include perioperative and postoperative vomiting or coughing, hypertension, orbital hemangiomas, orbital scarring, coagulopathy, and the use of platelet aggregation inhibitors.1 The major factors determining visual loss appear to be the mass effect of the retrobulbar hematoma on the optic nerve circulation and direct pressure neuropathy on the optic nerve itself.1,2
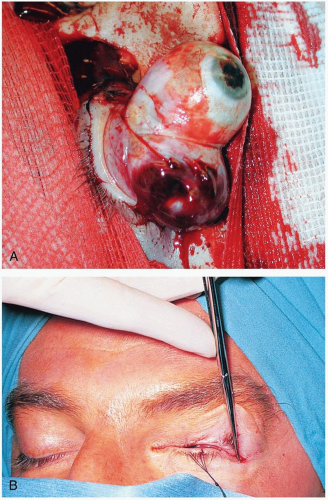 FIGURE 17-9 A: Gunshot wound to the head with severe proptosis due to retrobulbar hemorrhage. (Courtesy of Robert Chisolm, MD.) B: Lateral canthotomy. After a hemostat is placed horizontally over the lateral canthus for 1 minute, it is released, and sterile scissors are used to make a horizontal incision 1 cm toward the lateral orbital rim. (From Tasman, with permission.) |
Diagnosis
Retrobulbar hematoma is diagnosed clinically and confirmed by computed tomography, ultrasonography, or magnetic resonance imaging. Early signs include painful proptosis, decreased visual acuity, and occasionally scintillating scotomas.1,2 Late signs entail lid ecchymosis, chemosis, mydriasis, afferent pupillary defects, and ophthalmoplegia.2,3 The funduscopic examination is often normal but may show retinal pallor.1,2
Clinical Complications
Management
Treatment requires immediate ophthalmology consultation. In the absence of a visual deficit, medical interventions should suffice. These include ice packs, hypertension and pain control, bed rest, mannitol, acetazolamide parenteral steroids, and ocular hypotensive agents.1,2 If visual loss is present, immediate surgical decompression by any of a variety of approaches is necessary.1,2,3 In all cases, treatment should not be withheld while awaiting completion of imaging studies.1,2
REFERENCES
1. Wolfort FG, Vaughan TE, Wolfort SF, Nevarre DR. Retrobulbar hematoma and blepharoplasty. Plast Reconstr Surg 1999;104:2154-2162.
2. Ghufoor K, Sandhu G, Sutcliffe J. Delayed onset of retrobulbar haemorrhage following severe head injury: a case report and review. Injury 1998;29:139-141.
3. Korinth MC, Ince A, Banghard W, et al. Pterional orbita decompression in orbital hemorrhage and trauma. J Trauma 2002;53:73-78.
17-10 Nasal Bone Fracture
Matthew Spencer
Clinical Presentation
Patients present following trauma to the nose or face.
Pathophysiology
The nose is frequently exposed to trauma because of its central location and the fact that it protrudes from the face.1 The nasal bones are the most commonly fractured facial bone and the third most commonly fractured bone in the body.1 Because of the pliability of the pediatric bony architecture, children fracture their nasal bones less frequently than adults do; however, children have a higher rate of injury to the nasal septum.2
Diagnosis
A nasal fracture is a clinical diagnosis that can be confirmed with a plain lateral nasal radiograph of the face.1 There may be epistaxis in addition to nasal bridge swelling, tenderness, mobility, or crepitations.1 Patients may also have periorbital ecchymosis and swelling, and occasionally there is obvious external deviation, flattening, or broadening of the nose itself.1 The normal average intercanthal distance is 30 to 34 mm, but this may be increased when a fracture is present.1 Radiographs are not necessary if there is no significant deformity. The examining physician should always check for the presence of a septal hematoma, usually visible as a large purple bulge on one side of the septum. It is usually soft and easily compressed with a cotton swab, and it does not shrink after the application of vasoconstrictors.1
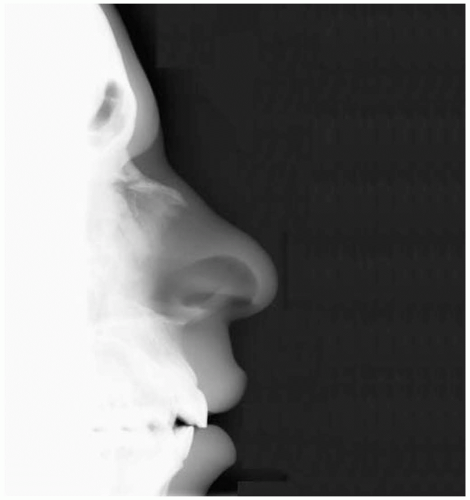 FIGURE 17-10 Minimally displaced fracture of the nasal bones. (Courtesy of Mark Silverberg, MD.) |
Clinical Complications
Management
If the injury is a simple nasal fracture with minor deformity, no immediate treatment is necessary. The patient may be discharged with analgesics and told to follow-up with an otolaryngology, oral surgery, or plastic surgery specialist in 48 to 72 hours.1 If there is a fixed nasal obstruction or severe cosmetic deformity, a subspecialty consultant should see the patient in the emergency department before discharge.1 If cerebrospinal fluid rhinorrhea is present, empiric antibiotics should be started promptly, and a neurosurgeon should be consulted.1
REFERENCES
1. Ellis E 3rd, Scott K. Assessment of patients with facial fractures. Emerg Med Clin North Am 2000;18:411-448.
2. Koltai PJ, Rabkin D. Management of facial trauma in children. Pediatr Clin North Am 1996;43:1253-1275.
17-11 C1-Skull Subluxation/Dislocation
Mohamed Badawy
Clinical Presentation
Patients with subluxation/dislocation of the skull on the first cervical vertebra (C1) often have concomitant head trauma and altered mental status. Such patients should be considered to have cervical spine injury until proven otherwise. The alert patient usually complains of upper neck or occipital pain. Patients may report a broad range of neurologic deficits that may include total paralysis.
Pathophysiology
C1-skull subluxation/dislocation refers to the abnormal disruption of the occipitoatlantal articulation, which may be partial (subluxation) or complete (dislocation).1 The occipitoatlantal junction is the transition between the cranial vault and the cervical spine. It is held together with strong ligamentous attachments. Combined hyperextension, distraction, and rotation results in either failure of the supporting ligaments or avulsion fractures of their insertions, with subsequent skull subluxation/dislocation. Children are more prone to dislocation, because of their smaller occipital condyles and the more horizontal plane of their craniocervical junction.2
 FIGURE 17-11 C1-skull subluxation/dislocation. (Courtesy of Mark Silverberg, MD.) |
Diagnosis
Meticulous examination of the entire spine is necessary, with focus on the status of the deep tendon reflexes, the presence of pathologic reflexes, and cranial nerve or sensory deficits.1 Cross-table lateral radiographs of the cervical spine should identify this injury. The “power ratio” is the ratio of the distance from the basion to the anterior edge of the posterior arch of the atlas versus the distance from the opisthion to the posterior portion of the anterior arch of the atlas.1 This ratio is used to assess the relationship between the occiput and the atlas and should be less than 0.9.1 A ratio of 1 or greater is considered abnormal.1 In addition, the distance between the basion and the dens should not exceed 10 mm in children and 5 mm in adults.1
Clinical Complications
Management
The treatment goals are to preserve neurologic function, reduce the subluxation/dislocation, and provide long-term spinal stability. Prehospital personnel should immobilize these patients before they are transported to the emergency department. Treatment in the hospital should focus on spinal immobilization and should involve neurosurgical or orthopedic spine consultations as quickly as possible after patient arrival. Halo vest placement and occipital cervical arthrodesis are often needed.1
REFERENCES
1. An HS. Cervical spine trauma. Spine 1998;23:2713-2729.
2. Montane I, Eismont FJ, Green BA. Traumatic occipitoatlantal dislocation. Spine 1991;16:112-116.
17-12 Dens Fractures
Edward Kim
Clinical Presentation
Patients with dens fractures (DFs) present after blunt trauma and hyperflexion/extension injuries, uniformly complaining of neck pain if they are awake. Patients may also report neurologic deficits such as numbness, paresthesias, or paralysis.1
Pathophysiology
Dens fractures account for almost 60% of all axis fractures and 10% to 18% of all cervical spine fractures.2 They can result from acute traumatic flexion or extension. In flexion injuries, anterior displacement of the dens may occur; in extension injuries, posterior displacement is more common.1 There are three classes of dens fractures. Type I is an avulsion of the tip of the odontoid; type II fractures obliquely traverse the body of the dens, and type III fractures extend into the body of the second cervical vertebra (C2).1,2
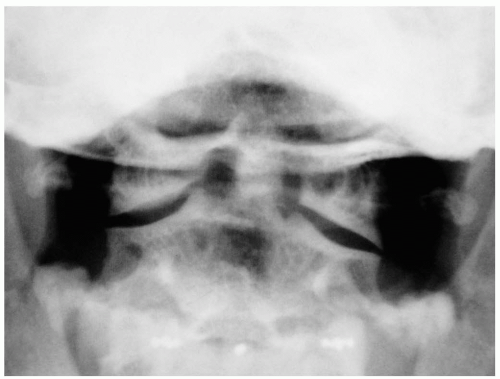 FIGURE 17-12 Type II dens fracture. (Courtesy of Mark Silverberg, MD.) |
Diagnosis
The diagnosis of a dens fracture may be suspected based on the history and physical examination findings; however, conventional radiography usually is needed to confirm its presence. The open-mouth odontoid film is the favored view to diagnose most dens fractures.1 However, helical computed tomography may be necessary if plain radiographs are inconclusive.2
Clinical Complications
Complications include neurologic injuries at the time of fracture and nonunion during the healing process.1,2 Late-onset progressive myelopathy may result from nonunion.2 Other complications include facet joint stiffness and loss of spinal alignment, both leading to cervical degenerative joint disease.2 Skin breakdown, pin site infections, and brain abscesses are potential complications of halo vest immobilization used in the treatment of dens fractures.2
Management
Treatment modalities depend on the grade of the fracture. Type I dens fractures require external immobilization with a halo vest for up to 12 weeks.1,2 Type II and III dens fractures are preferably managed nonoperatively but must be surgically corrected in cases with greater than 6 mm displacement, neurologic deficit, ventilator dependence, or nonunion after attempted nonoperative management.2
REFERENCES
1. An HS. Cervical spine trauma. Spine 1998;23:2713-2729.
2. Sasso RC. C2 dens fractures: treatment options. J Spinal Disord 2001;14:455-463.
17-13 Hangman’s Fracture
Oren Hirsch
Clinical Presentation
Patients with hangman’s fracture present with neck pain after an injury involving forced extension of the cervical spine. Inciting injuries commonly have high-energy mechanisms, such as falls, pedestrians being struck by an automobile, or high-speed motor vehicle collisions.1 On physical examination, cervical tenderness is almost always elicited. Patients may manifest neurologic deficits, depending on the severity of vertebral displacement and the presence of other cervical spine fractures.2
Pathophysiology
Hangman’s fracture, also known as traumatic spondylolisthesis of the axis, is a bilateral fracture of the pars interarticularis of the second cervical vertebra (C2).1 Judicial hangings, for which this fracture is named, result in hyperextension and distraction injury.1 However, the more common causes for this injury are motor vehicle collisions and falls, which produce the same fracture pattern through hyperextension and compression.1 The fracture line passes through the posterior elements, more specifically between the superior and inferior articular facets of C2.1
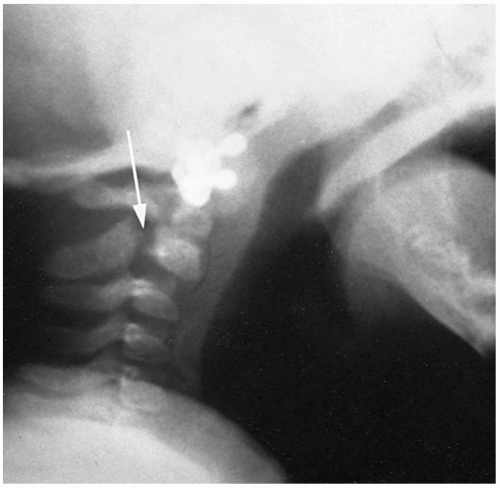 FIGURE 17-13 Hangman’s fracture. A 7-week-old infant with a fracture through the posterior elements of C2 (arrow). (From Sumchai A, Sternback G. Hangman’s fracture in a 7-week-old infant. Ann Emerg Med 1991;20:87, with permission.) |
Diagnosis
Plain cervical spine radiography, including lateral, anteroposterior, and odontoid views, should be obtained to confirm the diagnosis, although the lateral view is often diagnostic. Computed tomographic scanning may be helpful to delineate the precise pattern of bony injury and to visualize any possible intrusion into the spinal canal, indicating spinal cord involvement.1,2
Clinical Complications
Neurologic deficits secondary to concomitant intracranial injury or to spinal cord trauma may occur, particularly in cases of cervical vertebral subluxation. In addition, other cervical spine fractures may coexist and should be sought radiographically.2
Management
As in all patients with suspected cervical spine injuries, cervical immobilization with a rigid collar throughout the patient’s emergency department course is imperative. Standard advanced trauma life support (ATLS) protocols should be followed, because hangman’s fractures are often found in the setting of multisystem trauma. Individuals with hangman’s fractures require emergency, on-site neurosurgical consultation. Long-term treatment includes stabilization with a rigid cervical collar or a halo immobilization device.1 Surgical fusion usually is reserved for cases of fracture with severe angulation, disruption of the C2-C3 disk space, or failure of external immobilization to maintain fracture alignment.1
REFERENCES
1. Isolated fractures of the axis in adults. Neurosurgery 2002;50(3 Suppl):S125-S139.
2. Ryan MD, Henderson JJ. The epidemiology of fractures and fracture-dislocations of the cervical spine. Injury 1992;23:38-40.
17-14 Jefferson Burst Fracture
Oren Hirsch
Clinical Presentation
Patients with Jefferson burst fractures (JBFs) present with neck pain after an injury involving axial loading of the cervical spine. Associated neurologic complaints such as focal weakness, paralysis, or paresthesias may also be present.
Pathophysiology
A JBF is a combined anterior and posterior fracture of the atlas or first cervical vertebra (C1).1 Vertical compression forces are transmitted through the skull to the occipital condyles and onto the superior articular facets of the lateral masses of C1. The occipital condyles are downward sloping and act as a wedge to drive the ring-shaped atlas apart. Common mechanisms of injury include rollover motor vehicle collisions in which passengers are not wearing seatbelts, diving accidents, falls from height, and pedestrians being struck by motor vehicles.1
Diagnosis
Plain cervical spine radiography usually is adequate to confirm this diagnosis. Lateral, anteroposterior, and odontoid films should be obtained, but the open-mouth or odontoid view is the best projection to identify this fracture.1 In the setting of a suspected or evident fracture on the plain radiograph, a computed tomographic scan is recommended to delineate the precise pattern of bony injury. Magnetic resonance imaging is currently the modality of choice for diagnosing ligamentous disruption and associated spinal instability.2 On physical examination, cervical tenderness usually is present. Patients may manifest neurologic deficits, depending on the severity of the displacement of C1 on C2 or concomitant vertebral ligamentous injuries.1
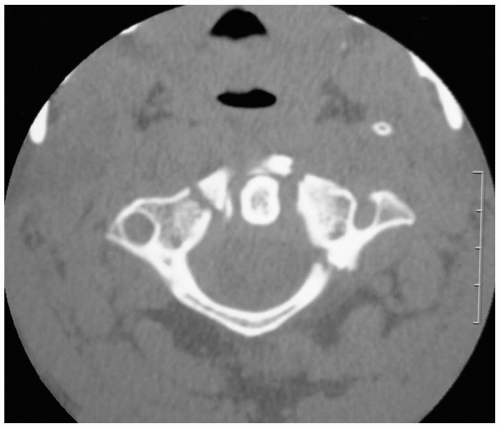 FIGURE 17-14 Computed tomogram showing vertebral “burst” fracture. (Courtesy of Mark Silverberg, MD.) |
Clinical Complications
Management
JBFs are found in the setting of multisystem trauma. Therefore, advanced trauma life support (ATLS) protocols should be strictly followed, including cervical immobilization with a rigid collar throughout the patient’s emergency department course. Individuals with JBFs require emergency neurosurgical consultation. Isolated stable Jefferson fractures should be treated with an external cervical immobilization device such as a rigid collar, suboccipital mandibular immobilizer brace, or halo ring-vest orthosis for 8 to 12 weeks. Unstable fractures with evidence of transverse atlantal ligamentous disruption should have either rigid immobilization alone with halo orthosis or surgical stabilization with vertebral fusion.1
REFERENCES
1. Isolated fractures of the atlas in adults. Neurosurgery 2002;50(3 Suppl):S120-S124.
2. Hadley MN, Dickman CA, Browner CM, Sonntag VK. Acute traumatic atlas fractures: management and long term outcome. Neurosurgery 1988;23:31-35.
17-15 Flexion Teardrop Fracture
Ian deSouza
Clinical Presentation
Patients with flexion teardrop fractures present after trauma with localized or generalized neck pain, paresthesia, paresis, or paralysis.1
Pathophysiology
A flexion teardrop fracture is a triangular fracture fragment at the anteroinferior corner of a cervical vertebral body.1 Flexion teardrop fractures result from forceful hyperflexion and compression applied to the anterior cervical spine when the flexed head strikes an object.2 In addition to the characteristic anteroinferior fracture, disruption of the anterior longitudinal ligament and intervertebral disk may occur. Equal and opposite posterior forces may lead to disruption of the posterior longitudinal ligament and facet joints. Posterior displacement of the vertebral body may result in compression of the anterior columns of the spinal cord and may be associated with substantial neurologic deficits.2
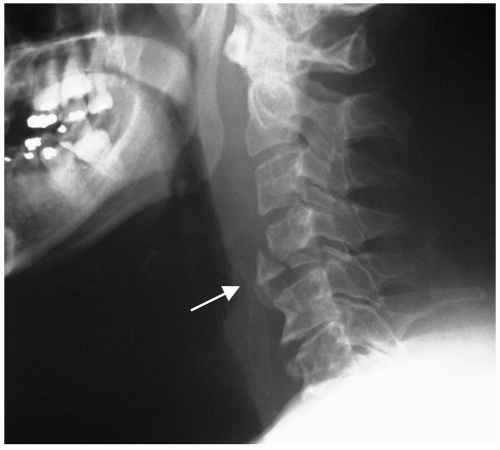 FIGURE 17-15 Anterior-inferior flexion fracture of the fourth cervical vertebra (C4). (Courtesy of Mark Silverberg, MD.) |
Diagnosis
The flexion teardrop fracture usually is obvious on plain radiographs, which demonstrate the anteroinferior “teardrop” fragment, posterior displacement of the vertebral body into the spinal canal, bilateral subluxation or dislocation of the facet joints, and widening or “fanning” of the interspinous spaces.1 Computed tomography or magnetic resonance imaging may be needed to fully define and delineate any ligamentous or spinal cord injury.1 Physical examination may reveal tenderness on palpation of the midline of the cervical spine, as well as findings consistent with the anterior cervical cord syndrome (ACS). The ACS involves complete quadriplegia with loss of pain, temperature, and some touch sensation combined with preservation of the posterior column functions, which include position, motion, and vibratory sense.3
Clinical Complications
Management
Because a flexion teardrop fracture is considered to be severely unstable, strict cervical spine immobilization is paramount.1,2,3 Emergency consultation with a neurosurgeon or orthopedic surgeon for spinal cord decompression, external immobilization, and eventual spinal fusion should be initiated as quickly as possible.2 The use of steroids in any case of spinal trauma should be considered but remains controversial.2
REFERENCES
1. Kim KS, Chen HH, Russel EJ, Rogers LF. Flexion teardrop fracture of the cervical spine: radiographic characteristics. AJR Am J Roentgenol 1989;152:319-326.
2. Petrie JG. Flexion injuries of the cervical spine. J Bone Joint Surg Am 1964;46;:1800-1806.
3. Schneider RC. The syndrome of acute anterior spinal cord injury. J Neurosurg 1955;12:95-122.
17-16 Extension Teardrop Fracture
Mohamed Badawy
Clinical Presentation
The extension teardrop fracture usually occurs in adults 40 to 70 years of age and only rarely in children.1 If awake and alert, patients usually complain of localized neck pain and tenderness. They may present with any type of spinal cord injury, although central cord syndrome (CCS) is the most common. CCS is characterized by weakness in the arms greater than in the legs, bladder dysfunction, and varying degrees of sensory loss below the level of the lesion.2
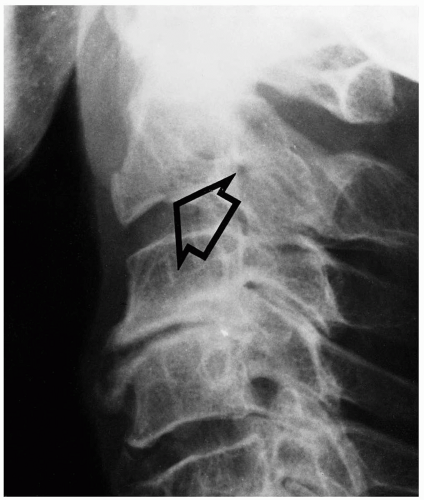 FIGURE 17-16 Extension teardrop fracture. The radiographic appearance of the classic extension teardrop fracture is an equilateral triangular avulsion fragment (open arrow) comprising the anteroinferior corner of the axis body. In elderly patients with osteoporosis, this fracture is associated with little or no prevertebral soft tissue swelling. (From Harris and Harris, with permission.) |
Pathophysiology
An extension teardrop fracture is characterized by avulsion of the inferior portion of the anterior part of a cervical vertebral body.1 This injury may result from a fall from heights or from high-speed trauma (e.g., motor vehicle crash). The mechanism is usually severe hyperextension of the neck. This mechanism applies tractional forces on the anterior longitudinal ligament at its insertion in the vertebral body.1 The anterior longitudinal ligament avulses the inferior corner of the vertebral body, resulting in this characteristic fracture pattern.1
Diagnosis
The avulsed anteroinferior portion of the vertebral body usually is visible on the lateral view of a standard cervical spine series. However, magnetic resonance imaging may provide more information by revealing associated spinal cord and other soft-tissue injuries.1
Clinical Complications
An extension teardrop fracture is stable when the head is in flexion but becomes unstable as the neck is extended. This may lead to transient or persistent neurologic deficits.1 High cervical-spine injuries may lead to death from diaphragm paralysis.
Management
Prehospital personnel should immobilize all patients with possible cervical spine injury before they are transported to the emergency department. As with all major traumatic injuries, the advanced trauma life support (ATLS) protocols should be followed. Because these neck injuries are potentially unstable, particular attention should be paid to cervical immobilization. Consultation should be sought on an emergency basis from a neurosurgery or orthopedics specialist. The use of steroids in trauma patients with neurologic deficits remains controversial.1,2
REFERENCES
1. Kiwerski J. Hyperextension-dislocation injuries of the cervical spine. Injury 1993;24:674-677.
2. Shneider RC, Thompson JM, Rebin J. The syndrome of acute central cervical spinal cord injury. J Neurol Neurosurg Psychiatry 1958;21:216-227.
17-17 Clay Shoveler’s Fracture
Ian deSouza
Clinical Presentation
Patients with clay shoveler’s fracture present with sudden onset of pain in the lower neck or between the shoulder blades that began while shoveling or lifting a heavy object.
Pathophysiology
Clay shoveler’s fracture involves an avulsion of the distal portion of one or more spinous processes of the lower cervical or upper thoracic vertebrae.1,2 The clay shoveler’s fracture was named after a frequent occupational injury among untrained workers who used long-handled shovels to toss soil 10 to 15 feet while draining swampy areas in Australia.1 Although its incidence has decreased since the advent of modern machinery, cases still occasionally arise from direct trauma in motor vehicle collisions and during sports.1 Such fractures have also been reported to occur after simple activities such as returning a barbell to its rack after heavy lifting.2 Fibers of the trapezius and rhomboid muscles originating from the posterior portion of the spinous processes in the lower neck vertebrae insert on the acromion, clavicle, and scapula and work to draw the scapula superomedially toward the spine. An avulsion fracture occurs when there is a sudden force on these muscles during forceful neck flexion or lifting by the arms.1
 FIGURE 17-17 Second and third cervical vertebrae (C2 and C3) fractures. (Courtesy of Robert Hendrickson, MD.) |
Diagnosis
The clay shoveler’s fracture may be suspected based on the history and physical examination, but it is diagnosed on plain radiographs of the cervical or upper thoracic spine.1 The anteroposterior view may reveal a “double shadow” of the spinous process, because the avulsed fragment is displaced inferiorly. Physical examination reveals tenderness to palpation of the affected spinous process, with overlying edema in some cases.1
Clinical Complications
Complications from these fractures are extremely rare but, when present, usually involve disability due to chronic pain or nonunion of the fracture fragments.2
Management
REFERENCES
1. Hakkal HG. Clay shoveler’s fracture. Am Fam Physician 1973;81:104-106.
2. Herrick RT. Clay-shoveler’s fracture in power-lifting: a case report. Am J Sports Med 1981;9:29-30.
17-18 Penetrating Neck Trauma
Melissa A. Eirich
Clinical Presentation
Pathophysiology
Injuries to the anterior neck can be divided into three zones. Zone 1 injuries are located below the level of the cricoid cartilage. Zone III is above the angles of the mandible, and zone II is between zones I and III.1
Diagnosis
Clinical Complications
Management
Advanced trauma life support (ATLS) protocols should be followed, but penetrating neck trauma requires special attention to airway evaluation. Zone I injuries are managed in the same manner as those caused by penetrating thoracic trauma. Zone II injuries that are symptomatic require surgical exploration with angiography. Treatment of asymptomatic zone II injuries is controversial; many surgeons explore these as well. If the wound is left unexplored and penetrated the platysma, these patients should undergo an angiogram to evaluate the neck vasculature, in addition to a bronchoscopy and esophagoscopy to evaluate the upper respiratory and gastrointestinal structures. Recent studies have shown that clinical examination alone misses only 1% of vascular injuries.2 Zone III injuries may include vascular injury, and angiography is recommended.3
REFERENCES
1. Peralta R, Hurford WE. Airway trauma. Int Anesthesiol Clin 2000; 38:111-127.
2. Sekharan J, Dennis JW, Veldenz HC, et al. Continued experience with physical examination alone for evaluation and management of penetrating zone two neck injuries: results of 145 cases. J Vasc Surg 2000;32:483-489.
3. Eddy VA. Is routine arteriography mandatory for penetrating injury to zone 1 of the neck? J Trauma 2000;48:208-214.
17-18 Penetrating Neck Trauma
Melissa A. Eirich
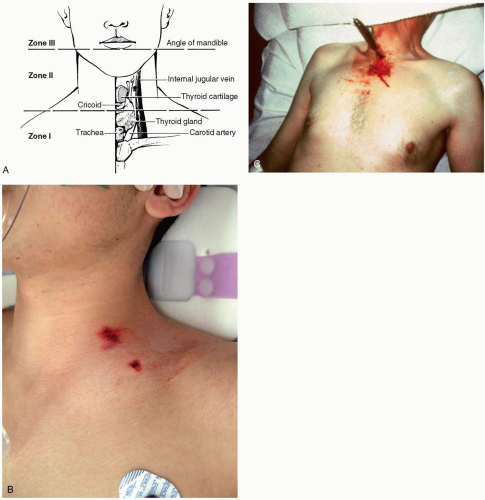 FIGURE 17-18 A: Anterior view of the neck. Significant structures and the zones of the neck are illustrated. (From Harwood-Nuss, with permission.) B: Gunshot wound in zone 1 of neck. (Courtesy of Mark Silverberg, MD.) C: Stab wound in zone 1 of neck. (Courtesy of Lewis J. Kaplan, MD.) |
17-19 Cervical Spine Subluxation
Madelyn Garcia
Clinical Presentation
Patients with cervical spine subluxation present after a flexion injury to the neck. Common mechanisms include unrestrained motor vehicle crashes and diving accidents.
Pathophysiology
Subluxation results from an anterior flexion pattern of injury, which accounts for approximately two thirds of all neck injuries.1 During extreme flexion, the posterior stabilizing ligaments are ruptured, and subluxation occurs with dislocation of the affected vertebrae anteriorly. In one series, subluxation without bony fracture accounted for 0.2% of cervical spine injuries.2 Most subluxation injuries are seen in young, athletic patients, but they may certainly occur in any age group.
Diagnosis
Signs and symptoms may be nonspecific and include pain, limitation of neck movement, and muscle spasm. Pain may be referred to the neck, scapula, shoulders, or upper arms and is often accompanied by finger paresthesias or numbness.1 In severe dislocations, the spinal cord can be injured, and patients often suffer transient neurologic symptoms that resolve before arrival at the emergency department. Definitive diagnosis is usually made on plain, three-view cervical spine series. Radiographic signs include localized kyphotic angulation of the cervical spine with or without anterior displacement (usually 1 to 3 mm) of the subluxed vertebra, altered configuration of interfaced joints, and “fanning” or widening of the spinous processes.3 Translations of greater than 3.5 mm and angulations of greater than 11 degrees are considered unstable. Subluxation must be distinguished from the “reversal of cervical lordosis” that is seen with muscle spasm. In subluxation, the kyphosis occurs at injured levels only, whereas in muscle spasm, it is diffuse. If there is any question on plain radiographic films, computed tomography or magnetic resonance imaging should be obtained to confirm the diagnosis.2
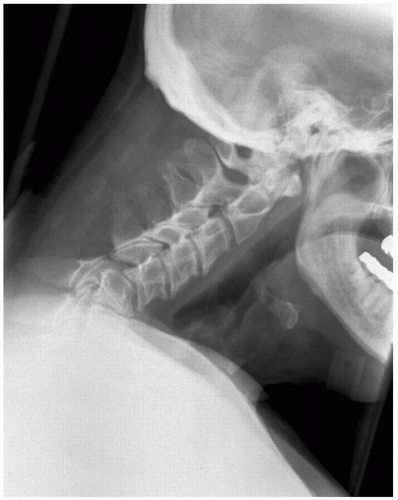 FIGURE 17-19 Subluxation of the fifth cervical vertebra (C5) on C6 with splaying of spinous processes. (Courtesy of Robert Hendrickson, MD.) |
Clinical Complications
Management
Careful spinal immobilization and orthopedic or neurosurgical consultation are essential. Most patients are treated with a cervical collar or brace for a minimum of 3 months to allow ligamentous healing, after which persistent symptoms may warrant cervical fusion or bone grafting.1
REFERENCES
1. Demetriades D, Charalambides K, Chahwan S, et al. Nonskeletal cervical spine injuries: epidemiology and diagnostic pitfalls. J Trauma 2000;48:724-727.
2. An HS. Cervical spine trauma. Spine 1998;23:2713-2729.
3. Green JD, Harle TS, Harris JH Jr. Anterior subluxation of the cervical spine: hyperflexion sprain. AJNR Am J Neuroradiol 1981;2:243-250.
17-20 Cervical Vertebral Compression Wedge Fracture
Mohamed Badawy
Clinical Presentation
Patients with wedge compression fractures usually present after head or neck trauma with localized tenderness over the injured vertebra.
Pathophysiology
A wedge compression fracture usually develops when a mild compressive force is combined with neck hyperflexion. The stability of these injuries depends on the integrity of the posterior longitudinal ligament complex. If the flexion force is more dominant than the compressive force, the posterior longitudinal complex may be disrupted with subsequent instability.1
 FIGURE 17-20 Sixth cervical (C6) vertebral compression fracture. (Courtesy of Robert Hendrickson, MD.) |
Diagnosis
Because this fracture tends to be stable, the neurologic examination is usually normal and nonfocal.1 A cross-table lateral radiograph of the cervical, thoracic, or lumbar regions (as required) usually identifies this injury. Buckling and loss of height of the anterior vertebral body cortex or disruption of the superior end-plate (or both) are indicative of this injury. With flexion forces of greater magnitude, the anterosuperior portion of the vertebral body may produce a separate fracture fragment.1 Prevertebral soft-tissue swelling, if present, usually is minimal and localized to the area of the involved segment. In the anteroposterior view, the involved vertebra may be normal or may reveal decreased vertical height. The absence of a vertical fracture of the vertebral body helps to distinguish the simple wedge fracture from the vertical compression fracture caused by axial loading.1,2
Clinical Complications
Complications of this injury are rare because of the fracture’s stability. However, if the posterior longitudinal ligament complex is disrupted, autonomic and neurologic deficits may be present.1
Management
As with all major traumatic injuries, advanced trauma life support (ATLS) protocols should be followed. Once the airway, breathing, and circulation have been evaluated and stabilized, the focus can be turned to the cervical spine. Treatment goals are to preserve neurologic function and to provide long-term spinal stability. In the emergency department, spinal stabilization should be maintained with a cervical collar. Consultation with a spine specialist should be obtained to coordinate further care and the need for long-term spinal immobilization.2
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


