Chapter 14 Trauma
Trauma in Australia and New Zealand is the leading cause of death in the first four decades of life. Fortunately, injury-related deaths have declined over the past 20 years; however, they continue to be a significant burden on health resources. The identification and management of seriously ill patients requires a coordinated approach that includes pre-hospital management, emergency management and definitive surgical care. The development of the Early Management of Severe Trauma Course and the Definitive Surgical Trauma Course, both available in Australia and New Zealand, has provided the platform for improved trauma management.
PRE-HOSPITAL TRIAGE
Pre-hospital assessment and management by ambulance services now enables the initial triage of patients to regional or major trauma services. The overriding goal is to get the right patient to the right hospital at the right time. Patients meeting the following criteria should be considered as having potentially life-threatening injuries requiring the services of an appropriately designated trauma centre. These criteria are also used by many hospitals as triggers to activate a trauma team response for an incoming patient, and include:
The definition of serious trauma to any body region includes the following.
PREPARATION
M Mechanism, e.g. fall, motor vehicle accident, pedestrian
I Injuries, e.g. abdominal tenderness, chest injury, fractured long bone
S Signs, e.g. pulse, systolic blood pressure, respiratory rate, conscious level
T Treatment, e.g. cervical spine immobilisation, oxygen, intravenous therapy, drugs
This information enables the trauma team to prepare and focus their attention on specific early interventions that may be life-saving for the given situation. For example, the multitrauma victim with abdominal injuries who remains hypotensive after 2 litres of intravenous fluids in the field will need uncrossmatched group O blood via a rapid warmer to be available on arrival and will probably require early transfer to the operating suite for definitive care.
PRIMARY SURVEY
3 Circulation and control of external haemorrhage
Examination
Assessment of a patient’s circulatory status does not require waiting for the blood pressure reading. Information gained from examination of the patient’s pulse, skin and level of consciousness is enough to make immediate resuscitation decisions, and the only equipment required is your eyes and your fingers. Remember to interpret your findings in the context of each individual you are assessing—the young, fit male who can compensate well despite considerable blood loss versus the elderly female with multiple comorbidities on numerous physiology-altering medications are two entirely different scenarios. Beware of patients who are hypotensive in the supine position—they have lost in excess of 30–40% of their blood volume and will require urgent resuscitation (Table 14.1).
Table 14.1 Estimated fluid and blood losses based on patient’s initial presentation (for a 70-kg patient)
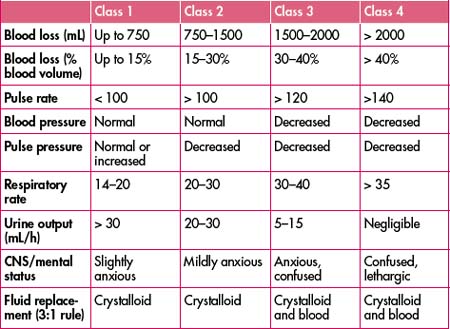
Level of consciousness. A decreased level of consciousness is an indicator of poor cerebral perfusion and, again, is presumed to be due to hypovolaemia until proven otherwise.
Priorities
Deteriorating haemodynamic status may be due to:
Major blood loss can occur from the following five sites:
Always remember, however, that the patient may bleed into multiple sites simultaneously, making such an ‘orderly’ assessment difficult in practical terms. The role of bedside ultrasonograpy as an adjunct to the clinical examination in the trauma patient has been developing for many years throughout the world and is rapidly expanding in Australia, replacing diagnostic peritoneal lavage in many centres. It has the advantage of being rapid, safe, non-invasive and, most importantly, repeatable.
Code Crimson activation can be simplified to the following four steps:
Remember: It is a rule-in test—if it is negative all bets are off.
4 Disability: brief neurological examination
All patients with a GCS of less than 12 should have aggressive ABC management, including consideration for early intubation. This will enable controlled ventilation/oxygenation and allow the team to focus on the circulatory status, thus attending to two key factors responsible for adverse outcomes in traumatic brain injury—hypoxaemia and hypotension.








