Toxicology Part 2: Specific Toxins
Shauna Jain
Introduction
Acetaminophen is the most common toxic ingestion seen in the emergency department
Tricyclic antidepressants are the most common fatal ingestion in children
Acetaminophen
Acetaminophen is metabolized by the liver; 5% is metabolized by cytochrome P450 to a toxic metabolite, N-actyl-para-benzoquinoneimine (NAPQI), which is reduced by glutathione to a nontoxic metabolite
In an overdose, glutathione stores are depleted and NAPQI causes liver toxicity
N-acetylcysteine (NAC) is given to eliminate NAPQI directly and indirectly by increasing glutathione levels
Clinical Presentation
1-24 hours: | Nausea, vomiting, anorexia |
24-48 hours: | RUQ pain, elevated liver enzymes and functions |
48-96 hours: | Peak hepatotoxicity, renal insufficiency, cerebral edema, coma, acidosis |
4-14 days: | Resolution of symptoms |
Evaluating Patients for Acetaminophen Toxicity
Acute Ingestion
Toxic dose: > 150 mg/kg acetaminophen
Measure serum level at 4 hours and evaluate on Rumack-Matthew nomogram
If patient presents 6-8 hours post ingestion, give NAC loading dose while waiting for level and continue NAC if acetaminophen level is toxic on nomogram
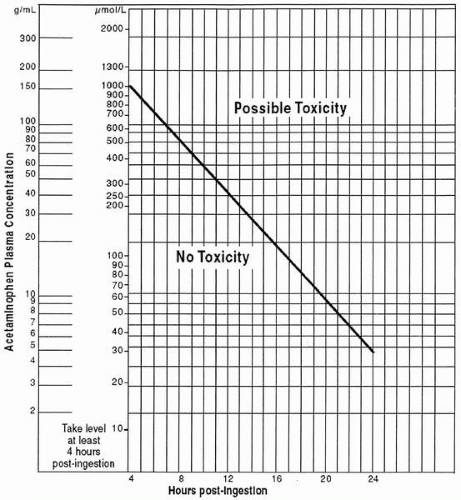 Figure 56.1 Rumack-Matthew Nomogram for Acetaminophen Toxicity Source: With permission from: Rumack-Matthew. Modified from: Rumack BH, Matthew H. Pediatrics 55, page 871 copyright 1975. |
Chronic Ingestion
Toxic dose: > 120 mg/kg/day acetaminophen
If a patient presents late and has detectable acetaminophen levels or elevated liver enzymes, consider to be at risk for a toxic ingestion
Treatment
Charcoal is given if the patient presents within 4 hours of ingestion and no contraindications
N-acetylcysteine (NAC) IV is given for a toxic ingestion:
Significant benefit of NAC even > 24 hours post toxic ingestion
Risk of anaphylactoid reaction, likely dependent on IV infusion rate
Two protocols available: 20- and 48-hour protocols
Oral NAC is available and has less risk of an allergic reaction
Supportive therapy
Salicylates
Salicylate toxicity results in uncoupling of oxidative phosphorylation and disruption of the Krebs cycle; decreases ATP production
Result is glycogenolysis, lipolysis, and anaerobic metabolism leading to hyperglycemia and metabolic acidosis
Respiratory alkalosis results from salicylates stimulating medulla to increase respiratory drive
Salicylate toxicity presents as a respiratory alkalosis with metabolic acidosis and initial hyperglycemia, then hypoglycemia
Clinical Presentation
Mild toxicity (150-300 mg/kg salicylates): vomiting, gastritis, tinnitus, tachypnea
Moderate toxicity (300-500 mg/kg salicylates): hyperthermia, diaphoresis, renal and liver dysfunction
Severe toxicity (> 500 mg/kg salicylates): coma, seizures, pulmonary edemaRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



